

A novel anti-HER2 anthracycline-based antibody-drug conjugate induces adaptive anti-tumor immunity and potentiates PD-1 blockade in breast cancer
- PMID: 30665463
- PMCID: PMC6341578
- DOI: 10.1186/s40425-018-0464-1
A novel anti-HER2 anthracycline-based antibody-drug conjugate induces adaptive anti-tumor immunity and potentiates PD-1 blockade in breast cancer
Abstract
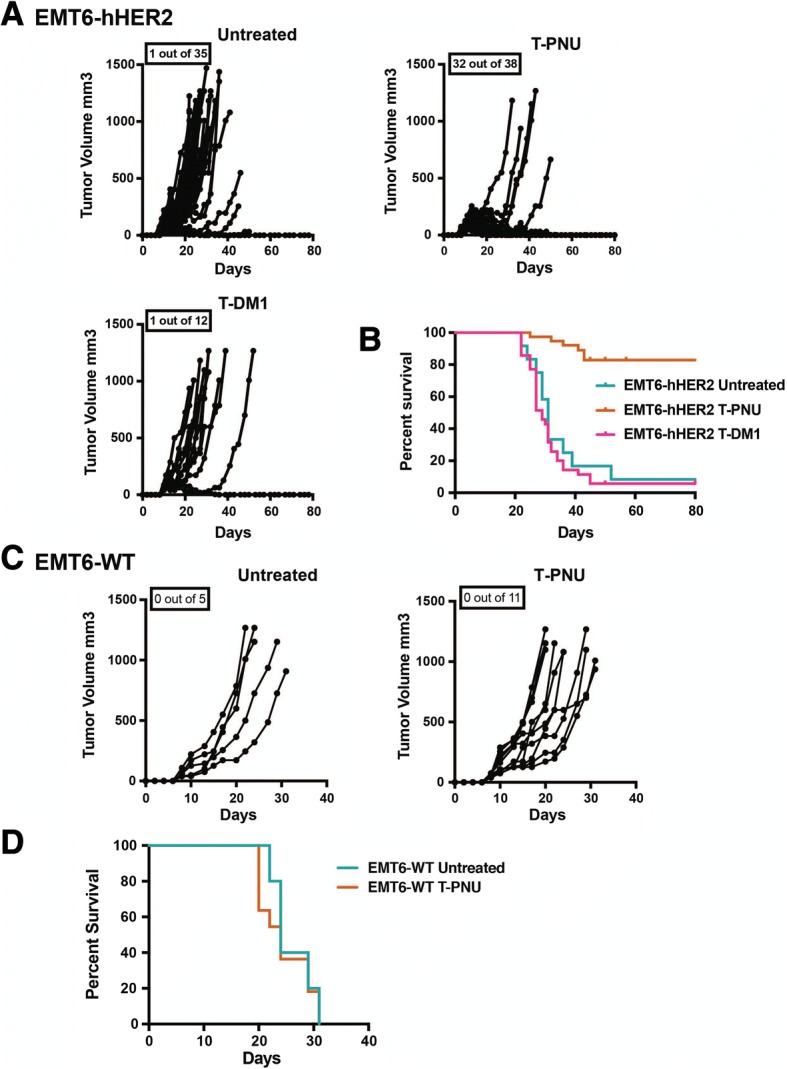
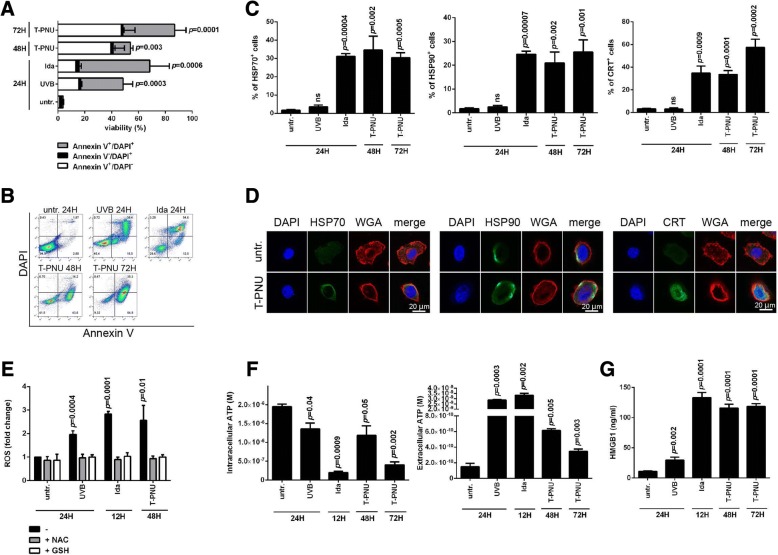
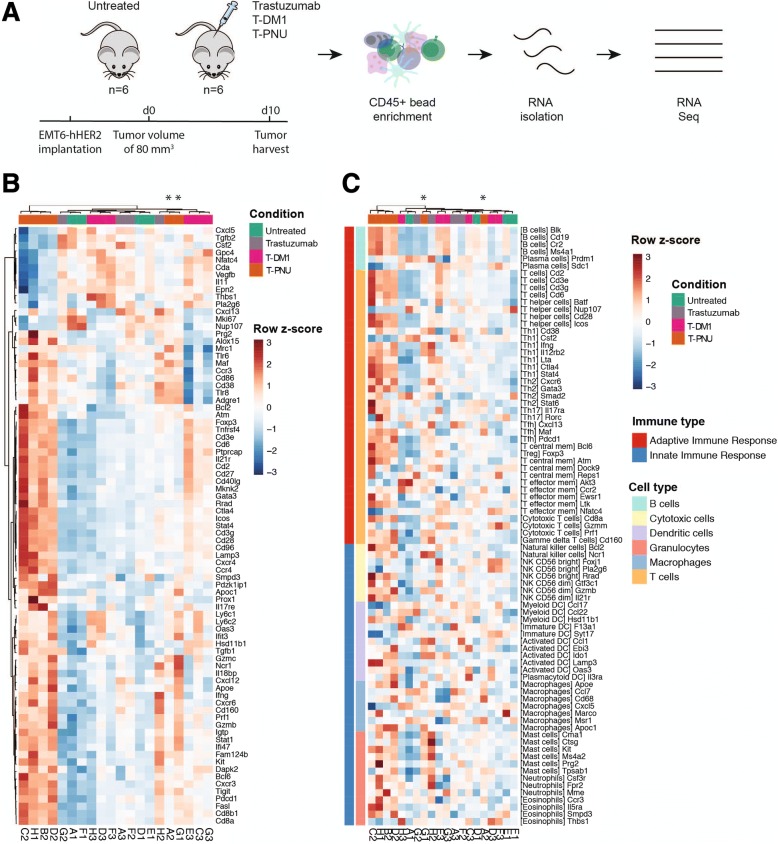
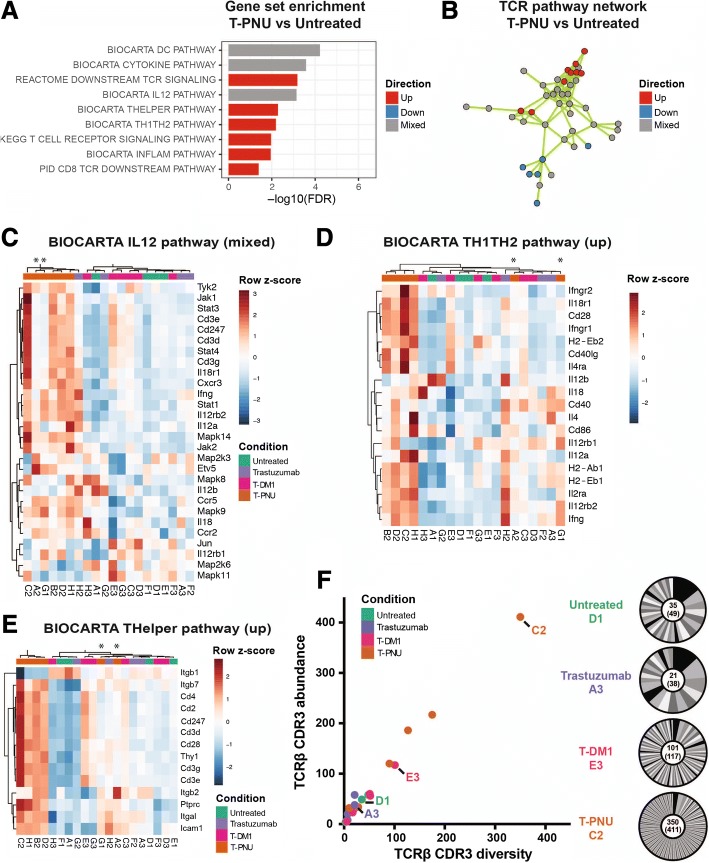
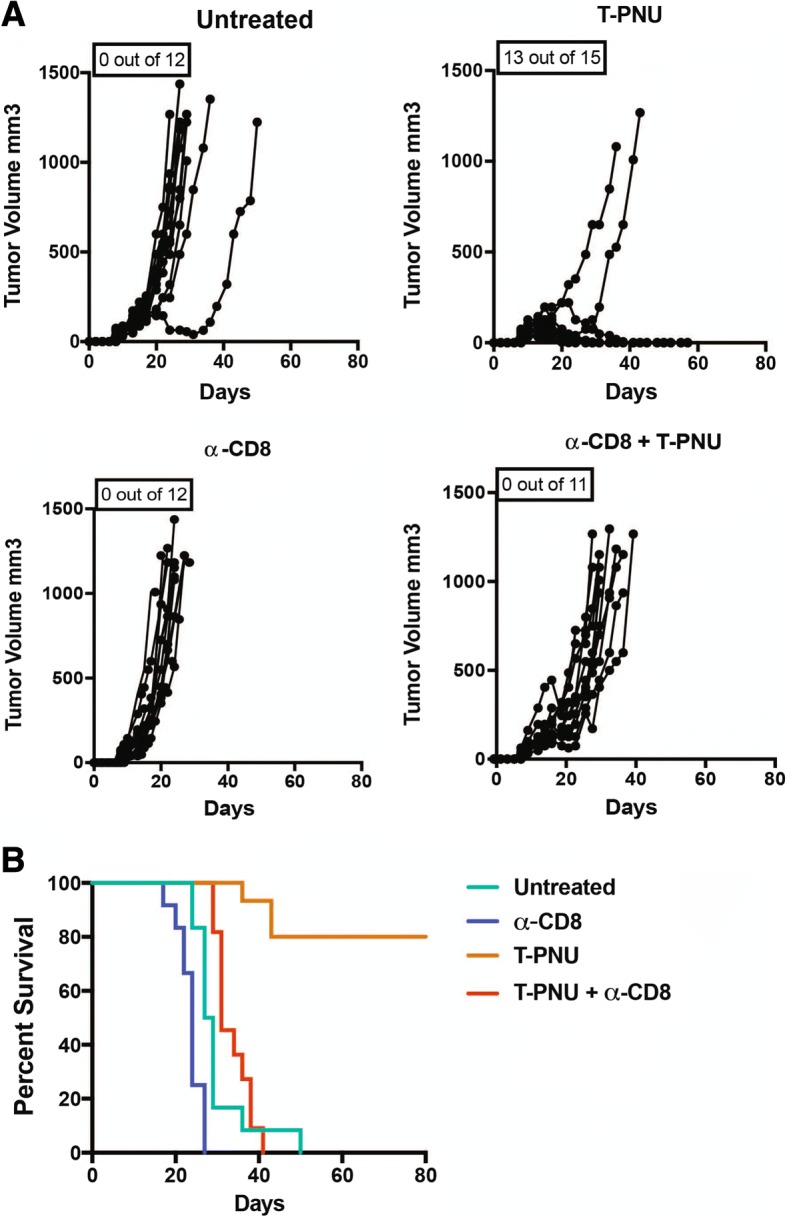
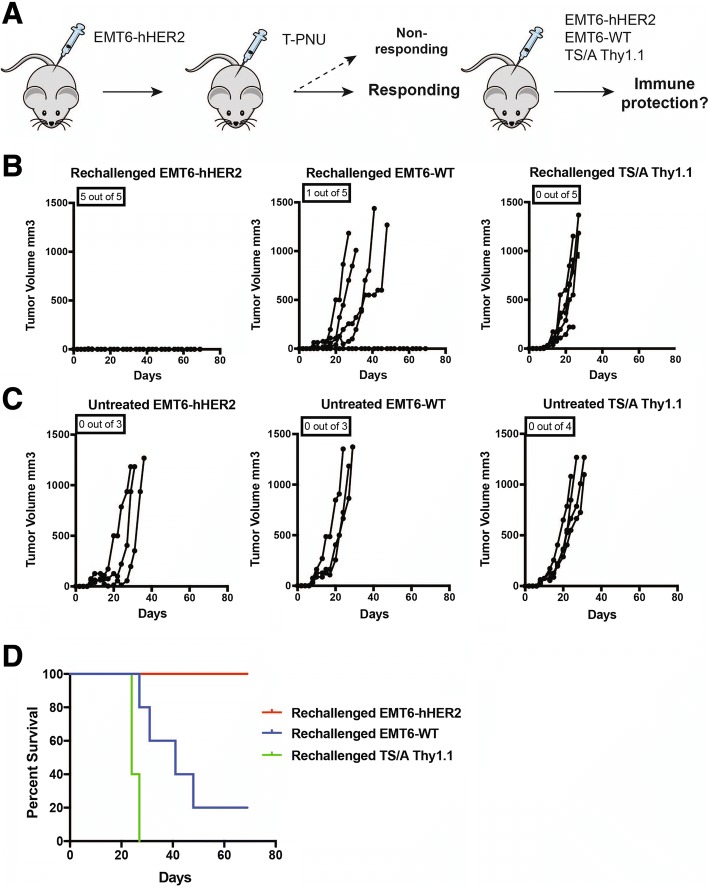
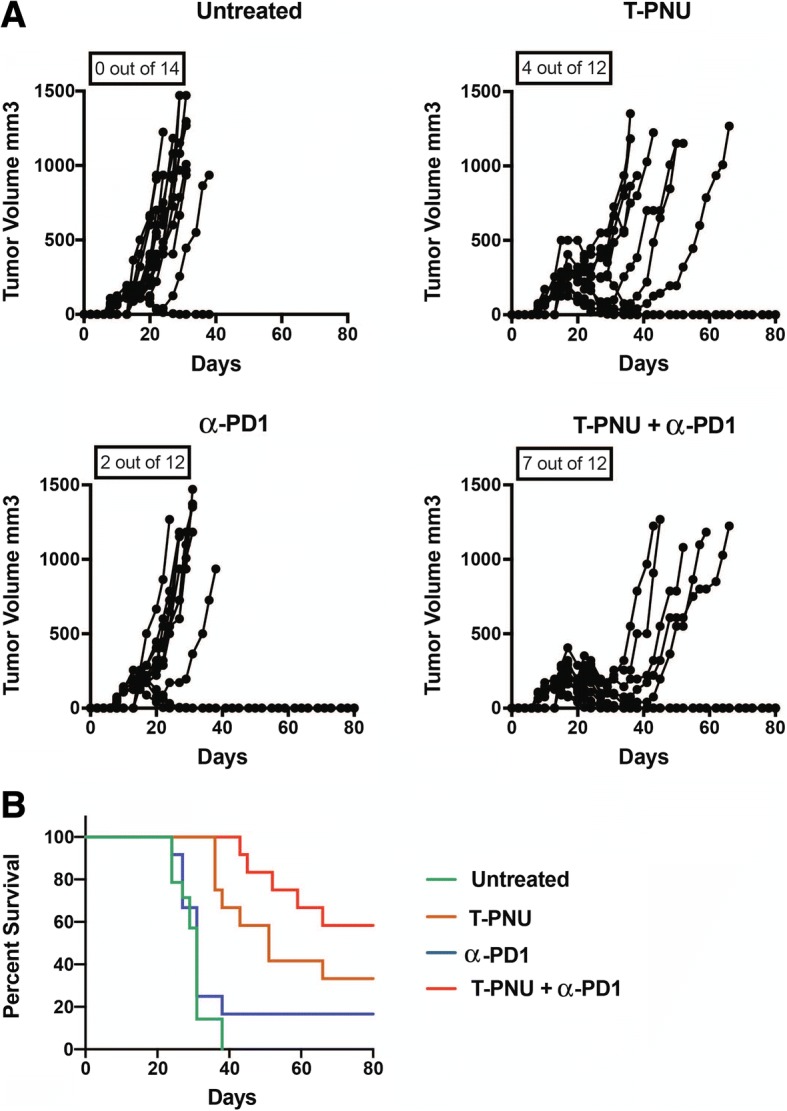
Increasing evidence suggests that antibody-drug conjugates (ADCs) can enhance anti-tumor immunity and improve clinical outcome. Here, we elucidate the therapeutic efficacy and immune-mediated mechanisms of a novel HER2-targeting ADC bearing a potent anthracycline derivate as payload (T-PNU) in a human HER2-expressing syngeneic breast cancer model resistant to trastuzumab and ado-trastuzumab emtansine. Mechanistically, the anthracycline component of the novel ADC induced immunogenic cell death leading to exposure and secretion of danger-associated molecular signals. RNA sequencing derived immunogenomic signatures and TCRβ clonotype analysis of tumor-infiltrating lymphocytes revealed a prominent role of the adaptive immune system in the regulation of T-PNU mediated anti-cancer activity. Depletion of CD8 T cells severely reduced T-PNU efficacy, thus confirming the role of cytotoxic T cells as drivers of the T-PNU mediated anti-tumor immune response. Furthermore, T-PNU therapy promoted immunological memory formation in tumor-bearing animals protecting those from tumor rechallenge. Finally, the combination of T-PNU and checkpoint inhibition, such as α-PD1, significantly enhanced tumor eradication following the treatment. In summary, a novel PNU-armed, HER2-targeting ADC elicited long-lasting immune protection in a murine orthotopic breast cancer model resistant to other HER2-directed therapies. Our findings delineate the therapeutic potential of this novel ADC payload and support its clinical development for breast cancer patients and potentially other HER2 expressing malignancies.
Keywords: Anthracycline; Antibody-drug conjugates; Checkpoint inhibitor combination therapy; HER2-positive breast cancer.
Conflict of interest statement
Ethics approval and consent to participate
Mice experiments have been conducted under the ethical approval of the Swiss Cantonal laws (License 2370/2480/2589).
Consent for publication
All authors concur with the content of submission and the material submitted for publication is not under consideration for publication elsewhere.
Competing interests
RB, RG, MB, TH, FW and UG are current or former employees of NBE-Therapeutics Ltd. No potential conflicts of interest were disclosed by the other authors.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Lewis Phillips GD, Li G, Dugger DL, Crocker LM, Parsons KL, Mai E, et al. Targeting HER2-positive breast cancer with trastuzumab-DM1, an antibody-cytotoxic drug conjugate. Cancer Res. American Association for Cancer Research. 2008;68:9280–9290. - PubMed
-
- Krop IE, Kim S-B, González-Martín A, LoRusso PM, Ferrero J-M, Smitt M, et al. Trastuzumab emtansine versus treatment of physician's choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15:689–699. doi: 10.1016/S1470-2045(14)70178-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous