

Timing of initiation of low-molecular-weight heparin administration in pregnant women with antiphospholipid syndrome: a randomized clinical trial of efficacy and safety
- PMID: 30666167
- PMCID: PMC6336021
- DOI: 10.2147/IJWH.S193293
Timing of initiation of low-molecular-weight heparin administration in pregnant women with antiphospholipid syndrome: a randomized clinical trial of efficacy and safety
Abstract
Objective: We aimed to evaluate the effect of different timing of initiation of low-molecular-weight heparin (LMWH) administration on the pregnancy outcomes in women with antiphospholipid syndrome (APS).
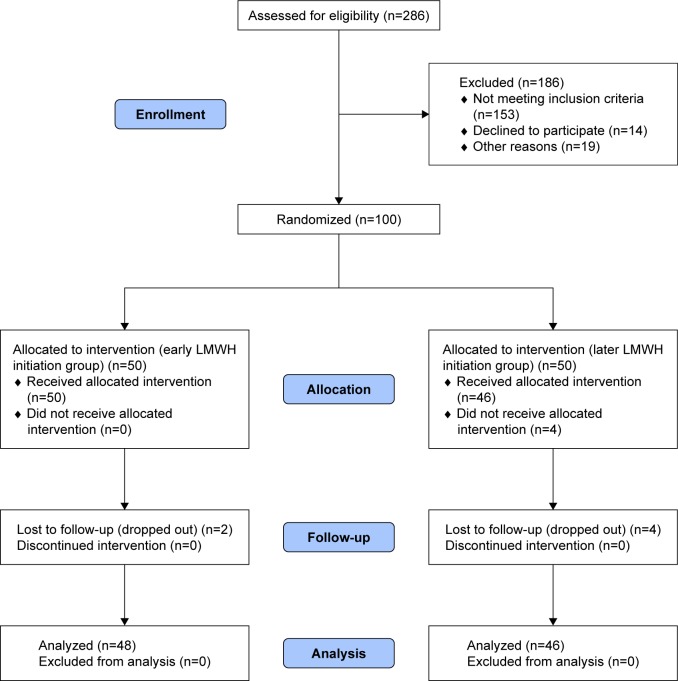
Materials and methods: A randomized controlled study was conducted on women with obstetrical APS. All participants were randomly divided at documentation of positive pregnancy test into two groups; early initiation group in which LMWH therapy was started once positive pregnancy test was established (in the fifth week of gestation), and later initiation group in which LMWH therapy was started after sonographic confirmation of fetal cardiac pulsation (in the seventh week of gestation). In both groups, LMWH (enoxaparin) was given at a dose of 40 mg/day subcutaneously and the therapy continued until end of pregnancy. The primary outcome measure was ongoing pregnancy rate and the secondary outcome measures were fetal loss, live birth rate, preterm labor before 34 weeks of gestation, intrauterine growth restriction (IUGR), and congenital fetal malformations.
Results: Ninety-four women (48 in the early initiation group and 46 in the later initiation group) were subjected to final analysis. The ongoing pregnancy rate was significantly higher in the early initiation group than in the later initiation group (81.2% vs 60.9%; P=0.040). However, both groups were similar in the incidences of fetal loss, preterm labor before 34 weeks of gestation, and IUGR, and live birth rate. No recorded congenital fetal malformations in both groups.
Conclusion: Early administration of LMWH for pregnant women with obstetrical APS reduces early pregnancy loss, but does not affect the incidence of late obstetrical complications.
Keywords: APS; LMWH; fetal loss.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Levine JS, Branch DW, Rauch J. The antiphospholipid syndrome. N Engl J Med. 2002;346(10):752–763. - PubMed
-
- Roubey RA. Immunology of the antiphospholipid antibody syndrome. Arthritis Rheum. 1996;39(9):1444–1454. - PubMed
-
- Alijotas-Reig J, Vilardell-Tarres M. Is obstetric antiphospholipid syndrome a primary nonthrombotic, proinflammatory, complement-mediated disorder related to antiphospholipid antibodies? Obstet Gynecol Surv. 2010;65(1):39–45. - PubMed
-
- Meroni PL, Raschi E, Camera M, et al. Endothelial activation by aPL: a potential pathogenetic mechanism for the clinical manifestations of the syndrome. J Autoimmun. 2000;15(2):237–240. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
