

Chronic fatigue syndrome in the emergency department
- PMID: 30666170
- PMCID: PMC6333158
- DOI: 10.2147/OAEM.S176843
Chronic fatigue syndrome in the emergency department
Abstract
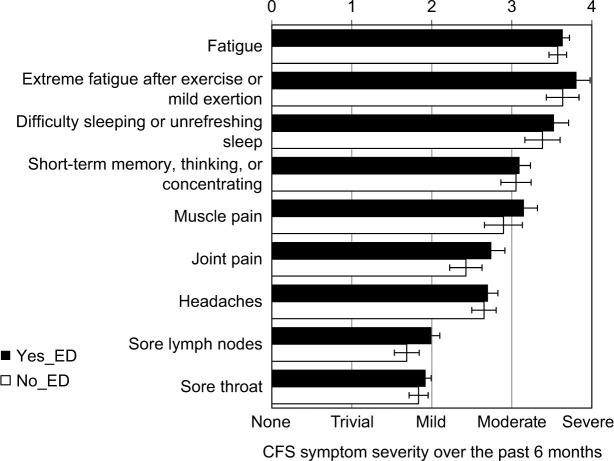
Purpose: Chronic fatigue syndrome (CFS) is a debilitating disease characterized by fatigue, postexertional malaise, cognitive dysfunction, sleep disturbances, and widespread pain. A pilot, online survey was used to determine the common presentations of CFS patients in the emergency department (ED) and attitudes about their encounters.
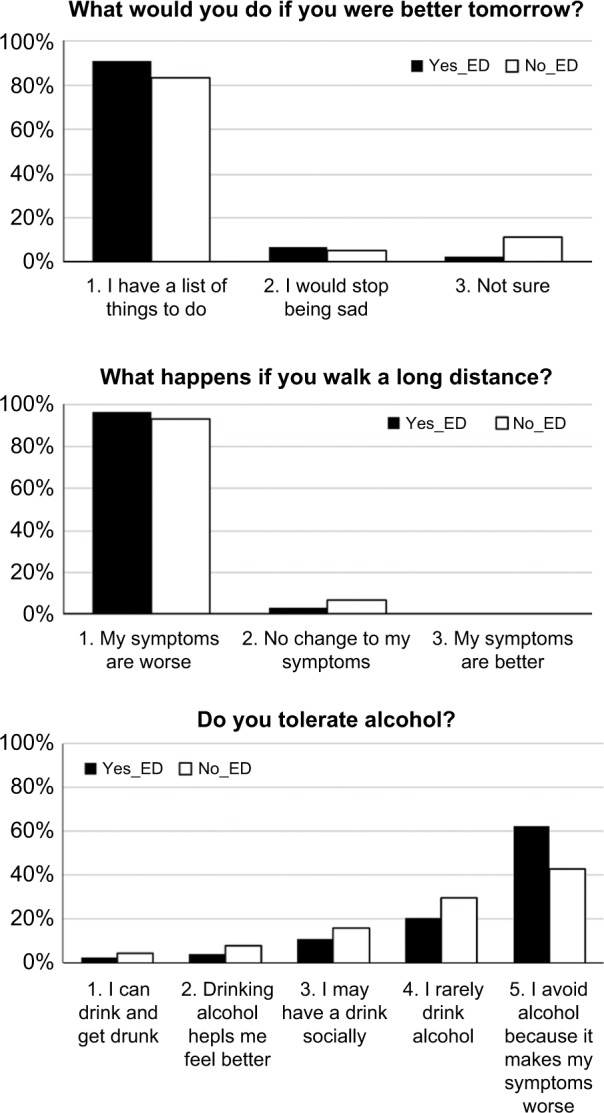
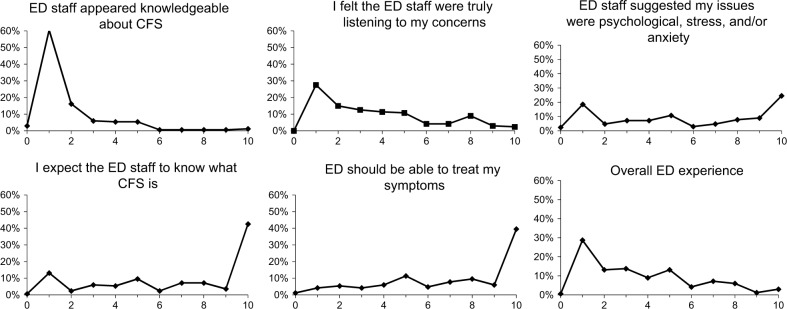
Methods: The anonymous survey was created to score the severity of core CFS symptoms, reasons for going to the ED, and Likert scales to grade attitudes and impressions of care. Open text fields were qualitatively categorized to determine common themes about encounters.
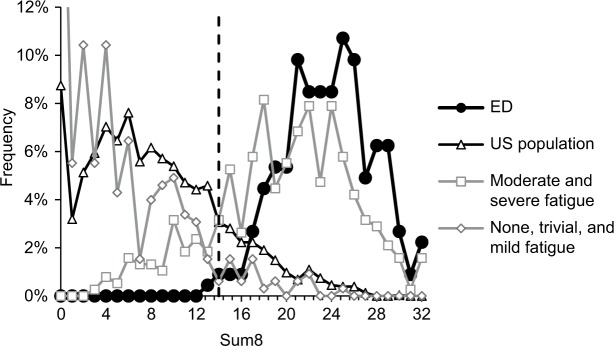
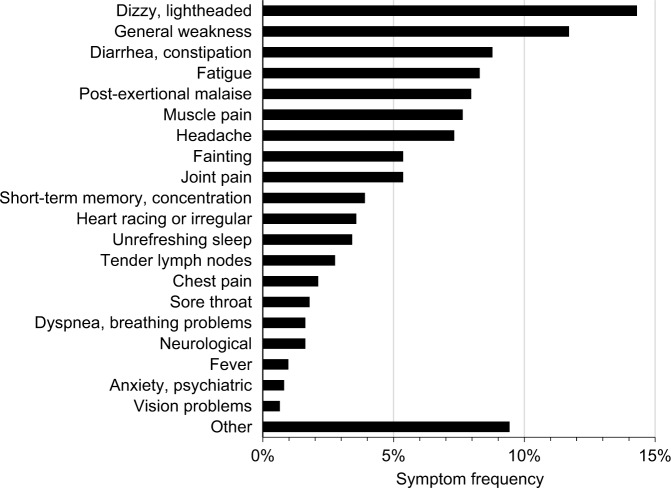
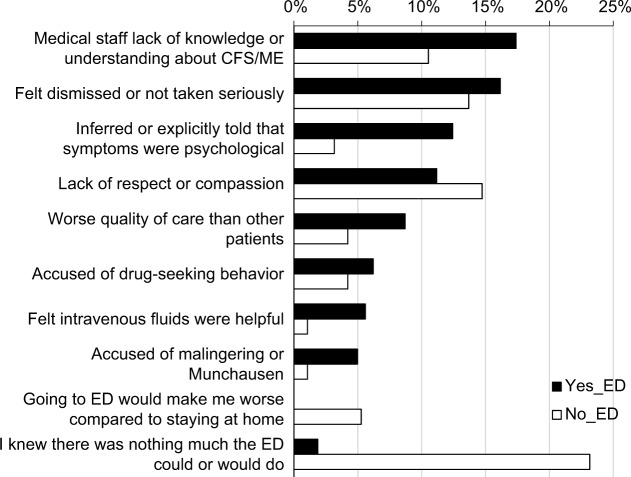
Results: Fifty-nine percent of respondents with physician-diagnosed CFS (total n=282) had gone to an ED. One-third of ED presentations were consistent with orthostatic intolerance; 42% of participants were dismissed as having psychosomatic complaints. ED staff were not knowledgeable about CFS. Encounters were unfavorable (3.6 on 10-point scale). The remaining 41% of subjects did not go to ED, stating nothing could be done or they would not be taken seriously. CFS subjects can be identified by a CFS questionnaire and the prolonged presence (>6 months) of unremitting fatigue, cognitive, sleep, and postexertional malaise problems.
Conclusion: This is the first investigation of the presentation of CFS in the ED and indicates the importance of orthostatic intolerance as the most frequent acute cause for a visit. The self-report CFS questionnaire may be useful as a screening instrument in the ED. Education of ED staff about modern concepts of CFS is necessary to improve patient and staff satisfaction. Guidance is provided for the diagnosis and treatment of CFS in these challenging encounters.
Keywords: SEID; myalgic encephalomyelitis; orthostatic intolerance; patient satisfaction; postexertional malaise; systemic exertion intolerance disease.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Numeric Rating Scales Show Prolonged Post-exertional Symptoms After Orthostatic Testing of Adults With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.Front Med (Lausanne). 2021 Jan 27;7:602894. doi: 10.3389/fmed.2020.602894. eCollection 2020. Front Med (Lausanne). 2021. PMID: 33585505 Free PMC article.
-
Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).J Transl Med. 2020 Jul 29;18(1):289. doi: 10.1186/s12967-020-02455-0. J Transl Med. 2020. PMID: 32727489 Free PMC article. Review.
-
Separating Patients with SEID from Those with CFS in the French ME/CFS Association, with Some Thoughts on Nomenclature.Diagnostics (Basel). 2022 Apr 27;12(5):1095. doi: 10.3390/diagnostics12051095. Diagnostics (Basel). 2022. PMID: 35626248 Free PMC article.
-
Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians.Rev Environ Health. 2015;30(4):223-49. doi: 10.1515/reveh-2015-0026. Rev Environ Health. 2015. PMID: 26613325 Review.
-
Submaximal Exercise Provokes Increased Activation of the Anterior Default Mode Network During the Resting State as a Biomarker of Postexertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.Front Neurosci. 2021 Dec 15;15:748426. doi: 10.3389/fnins.2021.748426. eCollection 2021. Front Neurosci. 2021. PMID: 34975370 Free PMC article.
Cited by
-
A National Survey of Children, Adults, and the Elderly in the Fourth Wave of the COVID-19 Pandemic to Compare Acute and Post-COVID-19 Conditions in Saudi Arabia.J Clin Med. 2023 Mar 14;12(6):2242. doi: 10.3390/jcm12062242. J Clin Med. 2023. PMID: 36983242 Free PMC article.
-
Comparison of three frailty measures for 90-day outcomes of elderly patients undergoing elective abdominal surgery.ANZ J Surg. 2021 Mar;91(3):335-340. doi: 10.1111/ans.16357. Epub 2020 Oct 5. ANZ J Surg. 2021. PMID: 33021042 Free PMC article.
-
Epstein-Barr virus-acquired immunodeficiency in myalgic encephalomyelitis-Is it present in long COVID?J Transl Med. 2023 Sep 17;21(1):633. doi: 10.1186/s12967-023-04515-7. J Transl Med. 2023. PMID: 37718435 Free PMC article. Review.
-
Virtual post-COVID-19 clinics in Saudi Arabia: navigating the effect of the pandemic with a national project.Front Public Health. 2025 Jul 30;13:1460324. doi: 10.3389/fpubh.2025.1460324. eCollection 2025. Front Public Health. 2025. PMID: 40809750 Free PMC article.
-
An Audit of UK Hospital Doctors' Knowledge and Experience of Myalgic Encephalomyelitis.Medicina (Kaunas). 2021 Aug 27;57(9):885. doi: 10.3390/medicina57090885. Medicina (Kaunas). 2021. PMID: 34577808 Free PMC article.
References
-
- Pitrou I, Lecourt AC, Bailly L, et al. Waiting time and assessment of patient satisfaction in a large reference Emergency Department: a prospective cohort study, France. Eur J Emerg Med. 2009;16(4):177–182. - PubMed
-
- Rhodes KV, Kushner HM, Bisgaier J, Prenoveau E. Characterizing Emergency Department discussions about depression. Acad Emerg Med. 2007;14(10):908–911. - PubMed
-
- Thompson DA, Yarnold PR, Williams DR, Adams SL. Effects of actual waiting time, perceived waiting time, information delivery, and expressive quality on patient satisfaction in the Emergency Department. Ann Emerg Med. 1996;28(6):657–665. - PubMed
-
- Krishel S, Baraff LJ. Effect of Emergency Department information on patient satisfaction. Ann Emerg Med. 1993;22(3):568–572. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
