

Epidural Spinal Cord Stimulation Facilitates Immediate Restoration of Dormant Motor and Autonomic Supraspinal Pathways after Chronic Neurologically Complete Spinal Cord Injury
- PMID: 30667299
- PMCID: PMC6648195
- DOI: 10.1089/neu.2018.6006
Epidural Spinal Cord Stimulation Facilitates Immediate Restoration of Dormant Motor and Autonomic Supraspinal Pathways after Chronic Neurologically Complete Spinal Cord Injury
Abstract
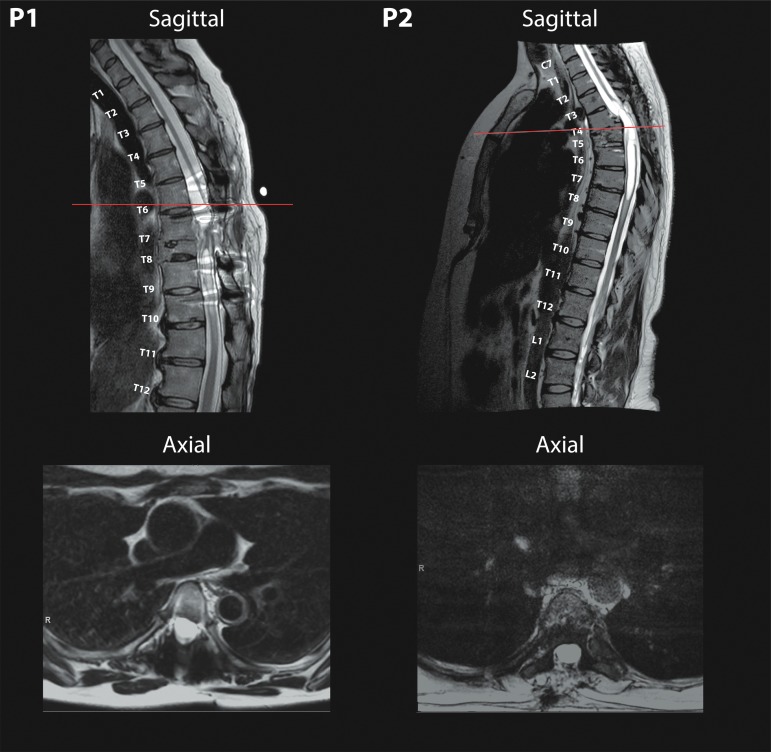
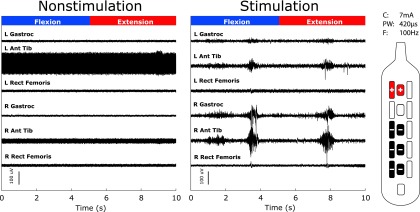
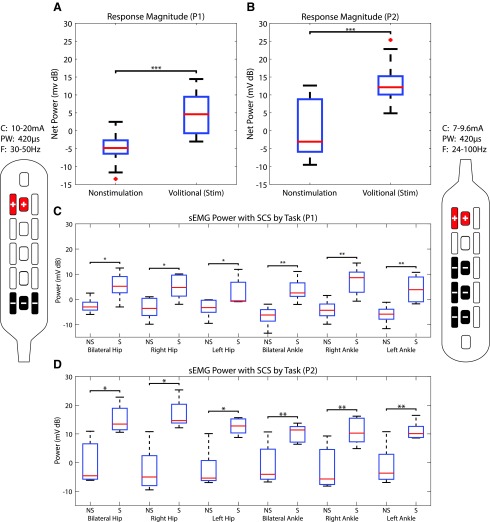
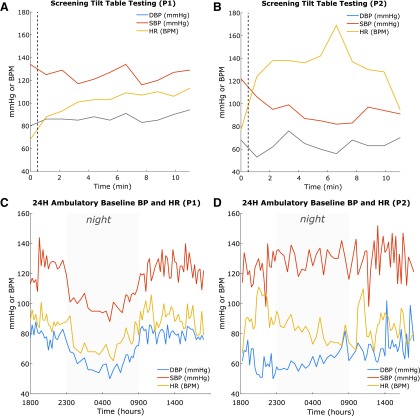
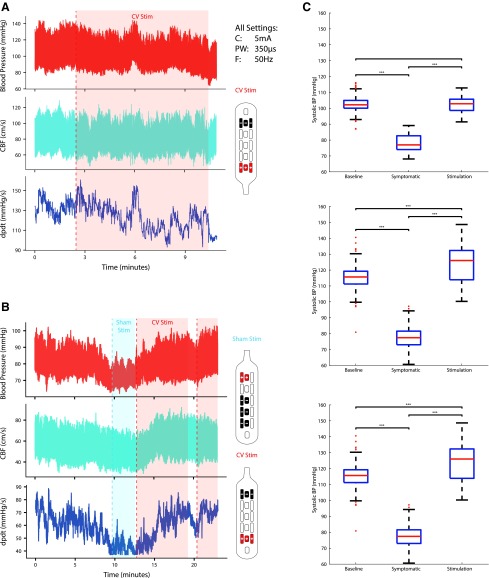
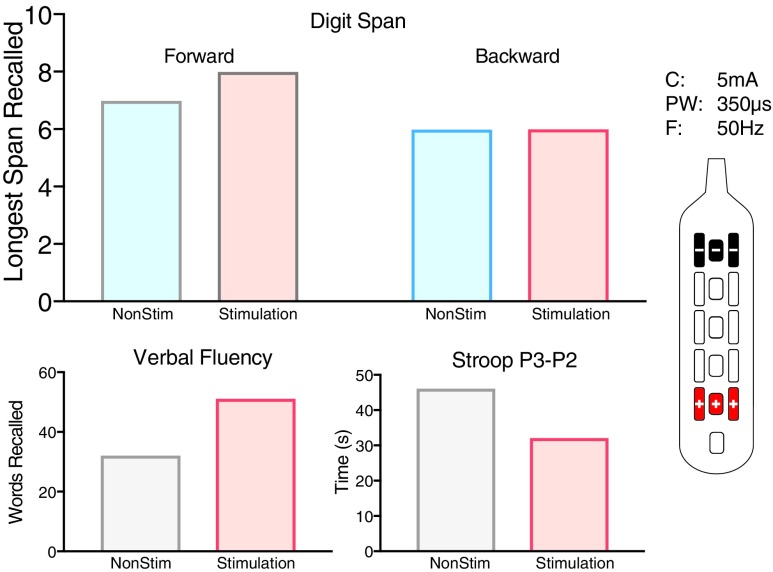
Epidural Spinal Cord Stimulation (eSCS) in combination with extensive rehabilitation has been reported to restore volitional movement in a select group of subjects after motor-complete spinal cord injury (SCI). Numerous questions about the generalizability of these findings to patients with longer term SCI have arisen, especially regarding the possibility of restoring autonomic function. To better understand the effect of eSCS on volitional movement and autonomic function, two female participants five and 10 years after injury at ages 48 and 52, respectively, with minimal spinal cord preservation on magnetic resonance imaging were implanted with an eSCS system at the vertebral T12 level. We demonstrated that eSCS can restore volitional movement immediately in two female participants in their fifth and sixth decade of life with motor and sensory-complete SCI, five and 10 years after sustaining severe radiographic injuries, and without prescribed or significant pre-habilitation. Both patients experienced significant improvements in surface electromyography power during a volitional control task with eSCS on. Cardiovascular function was also restored with eSCS in one participant with cardiovascular dysautonomia using specific eSCS settings during tilt challenge while not affecting function in a participant with normal cardiovascular function. Orgasm was achieved for the first time since injury in one participant with and immediately after eSCS. Bowel-bladder synergy improved in both participants while restoring volitional urination in one with eSCS. While numerous questions remain, the ability to restore some supraspinal control over motor function below the level of injury, cardiovascular function, sexual function, and bowel and bladder function should promote intense efforts to investigate and develop optimization strategies to maximize recovery in all participants with chronic SCI.
Keywords: autonomic; blood pressure; cardiovascular dysautonomia; spinal cord injury; spinal cord stimulation.
Conflict of interest statement
Dr. Darrow, Dr. Balser, Dr. Parr, and Dr. Samadani report a grant from MN State SCI/TBI Fund, grants from Abbott (Donation of Equipment) during the conduct of the study; Dr. Phillips and Dr. Krassioukov report grants from the Rick Hansen Institute during the conduct of the study. For Dr. Netoff, no competing financial interests exist.
Figures
References
-
- Shealy C.N., Mortimer J.T., and Reswick J.B. (1967). Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesth. Analg. 46, 489–491 - PubMed
-
- Shealy C.N., Mortimer J.T., and Hagfors N.R. (1970). Dorsal column electroanalgesia. J. Neurosurg. 32, 560–564 - PubMed
-
- Waltz J.M., Andreesen W.H., and Hunt D.P. (1987). Spinal cord stimulation and motor disorders. Pacing Clin. Electrophysiol. 10, 180–204 - PubMed
-
- Herman R., He J., D'Luzansky S., Willis W., and Dilli S. (2002). Spinal cord stimulation facilitates functional walking in a chronic, incomplete spinal cord injured. Spinal Cord 40, 65–68 - PubMed
-
- Harkema S., Gerasimenko Y., Hodes J., Burdick J., Angeli C., Chen Y., Ferreira C., Willhite A., Rejc E., Grossman R.G., and Edgerton V.R. (2011). Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: a case study. Lancet 377, 1938–1947 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical