

Automated Triaging of Adult Chest Radiographs with Deep Artificial Neural Networks
- PMID: 30667333
- PMCID: PMC6438359
- DOI: 10.1148/radiol.2018180921
Automated Triaging of Adult Chest Radiographs with Deep Artificial Neural Networks
Erratum in
-
Automated Triaging of Adult Chest Radiographs with Deep Artificial Neural Networks.Radiology. 2019 Apr;291(1):272. doi: 10.1148/radiol.2019194005. Radiology. 2019. PMID: 30897046 Free PMC article. No abstract available.
Abstract
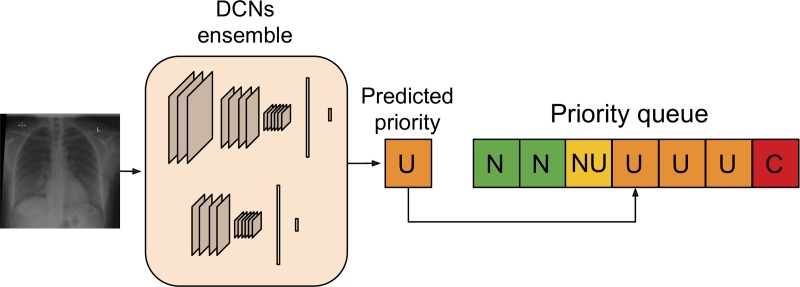
Purpose To develop and test an artificial intelligence (AI) system, based on deep convolutional neural networks (CNNs), for automated real-time triaging of adult chest radiographs on the basis of the urgency of imaging appearances. Materials and Methods An AI system was developed by using 470 388 fully anonymized institutional adult chest radiographs acquired from 2007 to 2017. The free-text radiology reports were preprocessed by using an in-house natural language processing (NLP) system modeling radiologic language. The NLP system analyzed the free-text report to prioritize each radiograph as critical, urgent, nonurgent, or normal. An AI system for computer vision using an ensemble of two deep CNNs was then trained by using labeled radiographs to predict the clinical priority from radiologic appearances only. The system's performance in radiograph prioritization was tested in a simulation by using an independent set of 15 887 radiographs. Prediction performance was assessed with the area under the receiver operating characteristic curve; sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were also determined. Nonparametric testing of the improvement in time to final report was determined at a nominal significance level of 5%. Results Normal chest radiographs were detected by our AI system with a sensitivity of 71%, specificity of 95%, PPV of 73%, and NPV of 94%. The average reporting delay was reduced from 11.2 to 2.7 days for critical imaging findings (P < .001) and from 7.6 to 4.1 days for urgent imaging findings (P < .001) in the simulation compared with historical data. Conclusion Automated real-time triaging of adult chest radiographs with use of an artificial intelligence system is feasible, with clinically acceptable performance. © RSNA, 2019 Online supplemental material is available for this article. See also the editorial by Auffermann in this issue.
Figures







Comment in
-
Automated Triaging of Adult Chest Radiographs.Radiology. 2019 Apr;291(1):203-204. doi: 10.1148/radiol.2019182909. Epub 2019 Jan 22. Radiology. 2019. PMID: 30667336 No abstract available.
References
-
- Geras KJ, Wolfson S, Kim SG, Moy L, Cho K. High-resolution breast cancer screening with multi-view deep convolutional neural networks. Cornell University Library; https://arxiv.org/abs/1703.07047. Published June 28, 2018. Accessed August 15, 2018.
-
- Lakhani P, Sundaram B. Deep learning at chest radiography: automated classification of pulmonary tuberculosis by using convolutional neural networks. Radiology 2017;284(2):574–582. - PubMed
-
- Rumelhart DE, Hinton GE, Williams RJ. Learning representations by back- propagating errors. Nature 1986;323(6088):533–536.
-
- LeCun Y, Bengio Y, Hinton G. Deep learning. Nature 2015;521(7553):436–444. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
