

Association of Time From Stroke Onset to Groin Puncture With Quality of Reperfusion After Mechanical Thrombectomy: A Meta-analysis of Individual Patient Data From 7 Randomized Clinical Trials
- PMID: 30667465
- PMCID: PMC6459219
- DOI: 10.1001/jamaneurol.2018.4510
Association of Time From Stroke Onset to Groin Puncture With Quality of Reperfusion After Mechanical Thrombectomy: A Meta-analysis of Individual Patient Data From 7 Randomized Clinical Trials
Erratum in
-
Error in Author Byline.JAMA Neurol. 2019 Jul 1;76(7):872. doi: 10.1001/jamaneurol.2019.1501. JAMA Neurol. 2019. PMID: 31135818 Free PMC article. No abstract available.
Abstract
Importance: Reperfusion is a key factor for clinical outcome in patients with acute ischemic stroke (AIS) treated with endovascular thrombectomy (EVT) for large-vessel intracranial occlusion. However, data are scarce on the association between the time from onset and reperfusion results.
Objective: To analyze the rate of reperfusion after EVT started at different intervals after symptom onset in patients with AIS.
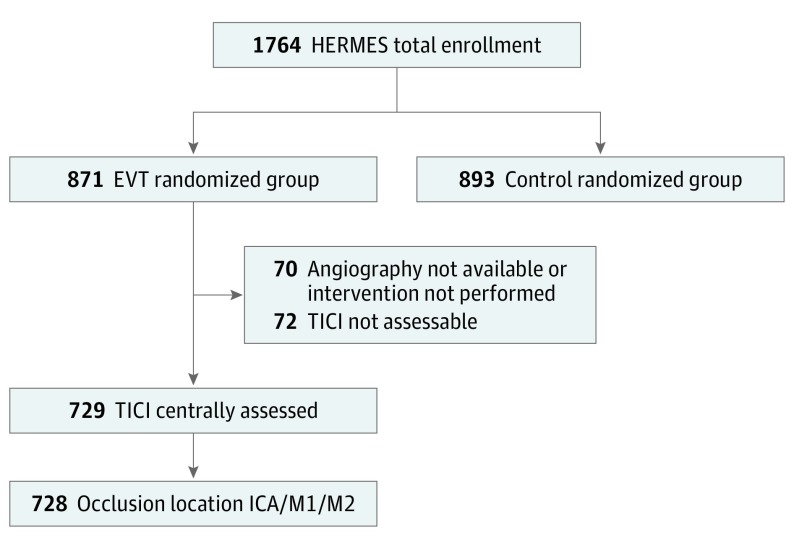
Design, setting, and participants: We conducted a meta-analysis of individual patient data from 7 randomized trials of the Highly Effective Reperfusion Using Multiple Endovascular Devices (HERMES) group. This is a multicenter cohort study of the intervention arm of randomized clinical trials included in the HERMES group. Patients with anterior circulation AIS who underwent EVT for M1/M2 or intracranial carotid artery occlusion were included. Each trial enrolled patients according to its specific inclusion and exclusion criteria. Data on patients eligible but not enrolled (eg, refusals or exclusions) were not available. All analyses were performed by the HERMES biostatistical core laboratory using the pooled database. Data were analyzed between December 2010 and April 2015.
Main outcomes and measures: Successful reperfusion was defined as a modified thrombolysis in cerebral infarction score of 2b/3 at the end of the EVT procedure adjusted for age, occlusion location, pretreatment intravenous thrombolysis, and clot burden score and was analyzed in relation to different intervals (onset, emergency department arrival, imaging, and puncture) using mixed-methods logistic regression.
Results: Among the 728 included patients, with a mean (SD) age of 65.4 (13.5) years and of whom 345 were female (47.4%), decreases in rates of successful reperfusion defined as a thrombolysis in cerebral infarction score of 2b/3 were observed with increasing time from admission or first imaging to groin puncture. The magnitude of effect was a 22% relative reduction (odds ratio, 0.78; 95% CI, 0.64-0.95) per additional hour between admission and puncture and a 26% relative reduction (odds ratio, 0.74; 95% CI, 0.59-0.93) per additional hour between imaging and puncture.
Conclusions and relevance: Because the probability of reperfusion declined significantly with time between hospital arrival and groin puncture, we provide additional arguments for minimizing the intervals after symptom onset in anterior circulation acute ischemic stroke.
Conflict of interest statement
Figures

References
-
- Higashida R, Furlan A, Roberts H, et al. ; Technology Assessment Committees of the American Society of Interventional and Therapeutic Neuroradiology and the Society of Interventional Radiology . Trial design and reporting standards for intraarterial cerebral thrombolysis for acute ischemic stroke. J Vasc Interv Radiol. 2003;14(9 Pt 2):S493-S494. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
