

Association of 30-Day Mortality With Oral Step-Down vs Continued Intravenous Therapy in Patients Hospitalized With Enterobacteriaceae Bacteremia
- PMID: 30667477
- PMCID: PMC6439703
- DOI: 10.1001/jamainternmed.2018.6226
Association of 30-Day Mortality With Oral Step-Down vs Continued Intravenous Therapy in Patients Hospitalized With Enterobacteriaceae Bacteremia
Erratum in
-
Error in Figure 3.JAMA Intern Med. 2019 Nov 1;179(11):1607. doi: 10.1001/jamainternmed.2019.5480. JAMA Intern Med. 2019. PMID: 31682686 Free PMC article. No abstract available.
Abstract
Importance: Conversion to oral therapy for Enterobacteriaceae bacteremia has the potential to improve the quality of life of patients by improving mobility, eliminating catheter-associated discomfort, decreasing the risk for noninfectious and infectious catheter-associated adverse events, and decreasing health care costs.
Objective: To compare the association of 30-day mortality with early oral step-down therapy vs continued parenteral therapy for the treatment of Enterobacteriaceae bloodstream infections.
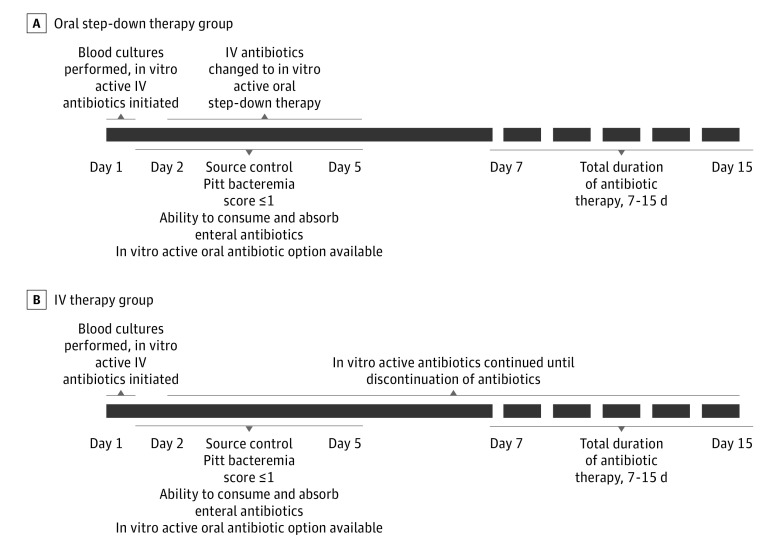
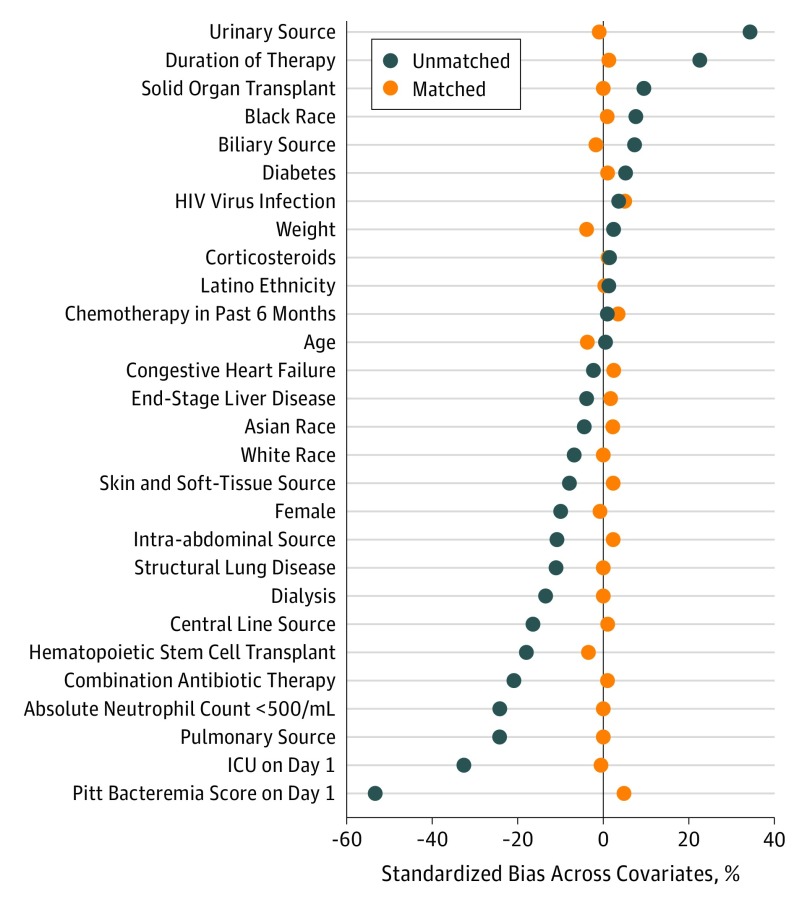
Design, setting, and participants: This retrospective multicenter cohort study included a 1:1 propensity score-matched cohort of 4967 unique patients hospitalized with monomicrobial Enterobacteriaceae bloodstream infection at 3 academic medical centers from January 1, 2008, through December 31, 2014. Eligibility criteria included appropriate source control measures, appropriate clinical response by day 5, active antibiotic therapy from day 1 until discontinuation of therapy, availability of an active oral antibiotic option, and ability to consume other oral medications or feeding. Statistical analysis was performed from March 2, 2018, to June 2, 2018.
Exposures: Oral step-down therapy within the first 5 days of treatment of Enterobacteriaceae bacteremia.
Main outcomes and measures: The main outcome was 30-day all-cause mortality.
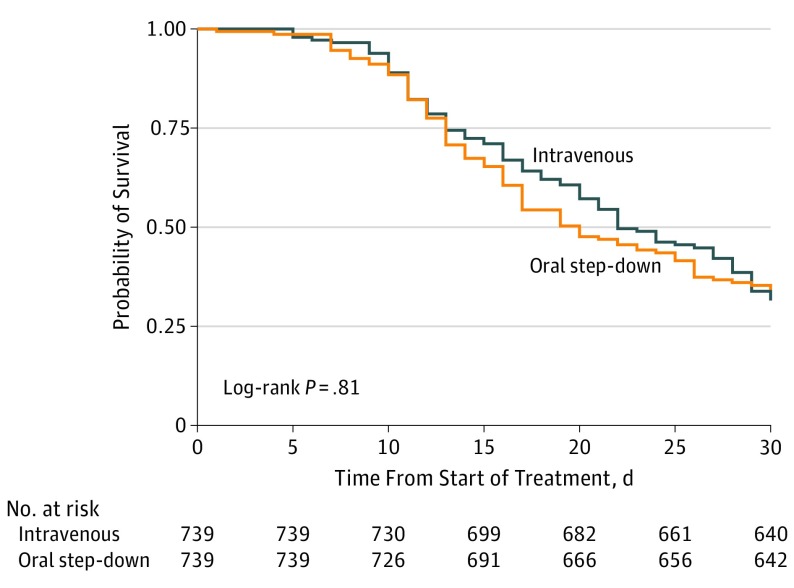
Results: Of the 2161 eligible patients, 1185 (54.8%) were male and 1075 (49.7%) were white; the median (interquartile range [IQR]) age was 59 (48-68) years. One-to-one propensity-score matching yielded 1478 patients, with 739 in each study arm. Sources of bacteremia included urine (594 patients [40.2%]), gastrointestinal tract (297 [20.1%]), central line-associated (272 [18.4%]), pulmonary (58 [3.9%]), and skin and soft tissue (41 [2.8%]). There were 97 (13.1%) deaths in the oral step-down group and 99 (13.4%) in the intravenous (IV) group within 30 days (hazard ratio [HR], 1.03; 95% CI, 0.82-1.30). There were no differences in recurrence of bacteremia within 30 days between the groups (IV, 6 [0.8%]; oral, 4 [0.5%]; HR, 0.82 [0.33-2.01]). Patients transitioned to oral step-down therapy were discharged from the hospital an average of 2 days (IQR, 1-6) sooner than patients who continued to receive IV therapy (5 days [IQR, 3-8 days] vs 7 days [IQR, 4-14 days]; P < .001).
Conclusions and relevance: In this study, 30-day mortality was not different among hospitalized patients who received oral step-down vs continued parenteral therapy for the treatment of Enterobacteriaceae bloodstream infections. The findings suggest that transitioning to oral step-down therapy may be an effective treatment approach for patients with Enterobacteriaceae bacteremia who have received source control and demonstrated an appropriate clinical response. Early transition to oral step-down therapy may be associated with a decrease in the duration of hospital stay for patients with Enterobacteriaceae bloodstream infections.
Conflict of interest statement
Figures
Comment in
-
Power Calculations, Effect Sizes, and 30-Day Mortality in Enterobacteriaceae Bacteremia.JAMA Intern Med. 2019 Jun 1;179(6):849-850. doi: 10.1001/jamainternmed.2019.1190. JAMA Intern Med. 2019. PMID: 31157843 No abstract available.
References
-
- Mermel LA, Allon M, Bouza E, et al. . Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America [published correction appears in Clin Infect Dis. 2010;50(7):1079]. Clin Infect Dis. 2009;49(1):1-45. doi:10.1086/599376 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
