

Association of Aspirin Use for Primary Prevention With Cardiovascular Events and Bleeding Events: A Systematic Review and Meta-analysis
- PMID: 30667501
- PMCID: PMC6439678
- DOI: 10.1001/jama.2018.20578
Association of Aspirin Use for Primary Prevention With Cardiovascular Events and Bleeding Events: A Systematic Review and Meta-analysis
Erratum in
-
Errors in Results.JAMA. 2019 Jun 11;321(22):2245. doi: 10.1001/jama.2019.3941. JAMA. 2019. PMID: 31184719 Free PMC article. No abstract available.
Abstract
Importance: The role for aspirin in cardiovascular primary prevention remains controversial, with potential benefits limited by an increased bleeding risk.
Objective: To assess the association of aspirin use for primary prevention with cardiovascular events and bleeding.
Data sources: PubMed and Embase were searched on Cochrane Library Central Register of Controlled Trials from the earliest available date through November 1, 2018.
Study selection: Randomized clinical trials enrolling at least 1000 participants with no known cardiovascular disease and a follow-up of at least 12 months were included. Included studies compared aspirin use with no aspirin (placebo or no treatment).
Data extraction and synthesis: Data were screened and extracted independently by both investigators. Bayesian and frequentist meta-analyses were performed.
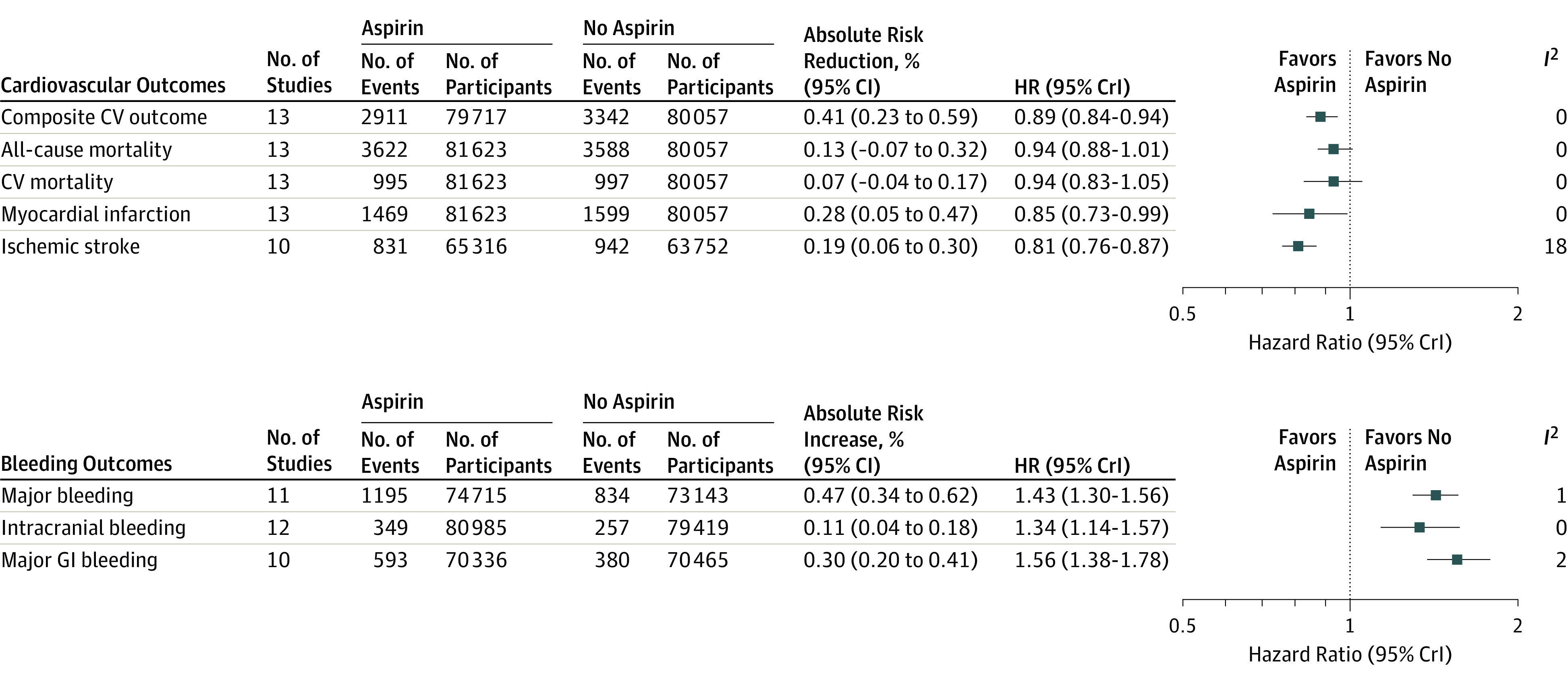
Main outcomes and measures: The primary cardiovascular outcome was a composite of cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke. The primary bleeding outcome was any major bleeding (defined by the individual studies).
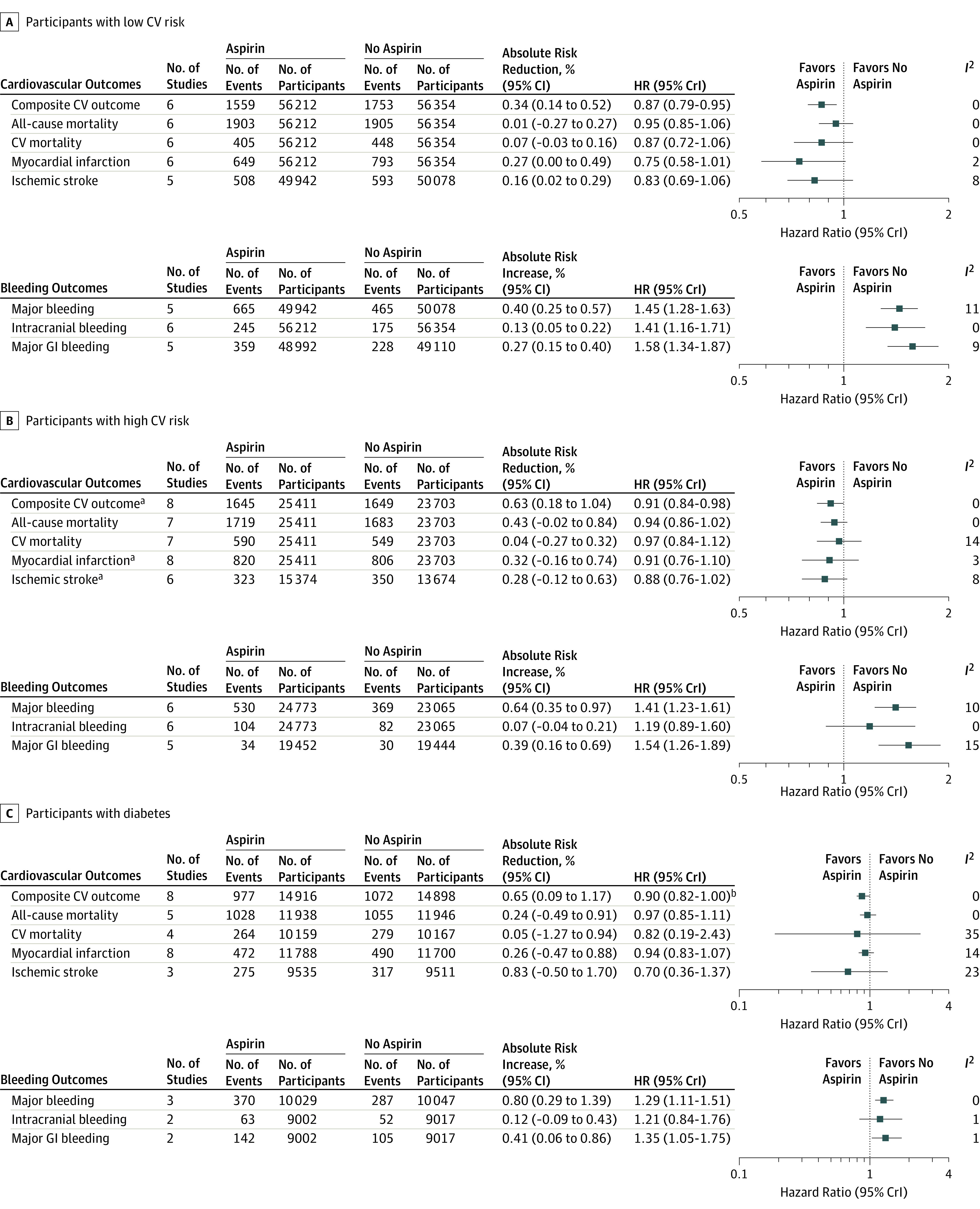
Results: A total of 13 trials randomizing 164 225 participants with 1 050 511 participant-years of follow-up were included. The median age of trial participants was 62 years (range, 53-74), 77 501 (47%) were men, 30 361 (19%) had diabetes, and the median baseline risk of the primary cardiovascular outcome was 9.2% (range, 2.6%-15.9%). Aspirin use was associated with significant reductions in the composite cardiovascular outcome compared with no aspirin (57.1 per 10 000 participant-years with aspirin and 61.4 per 10 000 participant-years with no aspirin) (hazard ratio [HR], 0.89 [95% credible interval, 0.84-0.95]; absolute risk reduction, 0.38% [95% CI, 0.20%-0.55%]; number needed to treat, 265). Aspirin use was associated with an increased risk of major bleeding events compared with no aspirin (23.1 per 10 000 participant-years with aspirin and 16.4 per 10 000 participant-years with no aspirin) (HR, 1.43 [95% credible interval, 1.30-1.56]; absolute risk increase, 0.47% [95% CI, 0.34%-0.62%]; number needed to harm, 210).
Conclusions and relevance: The use of aspirin in individuals without cardiovascular disease was associated with a lower risk of cardiovascular events and an increased risk of major bleeding. This information may inform discussions with patients about aspirin for primary prevention of cardiovascular events and bleeding.
Conflict of interest statement
Figures
Comment in
-
Aspirin for Primary Prevention: Clinical Considerations in 2019.JAMA. 2019 Jan 22;321(3):253-255. doi: 10.1001/jama.2018.20577. JAMA. 2019. PMID: 30667488 No abstract available.
-
Review: In adults without CVD, aspirin reduces CV events and increases major bleeding compared with no aspirin.Ann Intern Med. 2019 May 21;170(10):JC53. doi: 10.7326/ACPJ201905210-053. Ann Intern Med. 2019. PMID: 31108515 No abstract available.
-
Meta-analysis of Aspirin for Primary Prevention of Cardiovascular Events.JAMA. 2019 Jun 11;321(22):2243-2244. doi: 10.1001/jama.2019.4005. JAMA. 2019. PMID: 31184732 No abstract available.
-
Meta-analysis of Aspirin for Primary Prevention of Cardiovascular Events.JAMA. 2019 Jun 11;321(22):2244. doi: 10.1001/jama.2019.4013. JAMA. 2019. PMID: 31184734 No abstract available.
References
-
- Antithrombotic Trialists’ (ATT) Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849-1860. doi: 10.1016/S0140-6736(09)60503-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
