

Routine orthostatic LVOT gradient assessment in patients with basal septal hypertrophy and LVOT flow acceleration at rest: please stand up
- PMID: 30668520
- PMCID: PMC6391932
- DOI: 10.1530/ERP-18-0072
Routine orthostatic LVOT gradient assessment in patients with basal septal hypertrophy and LVOT flow acceleration at rest: please stand up
Abstract
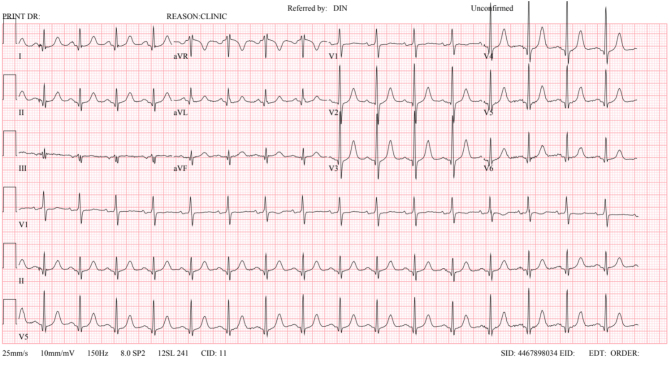
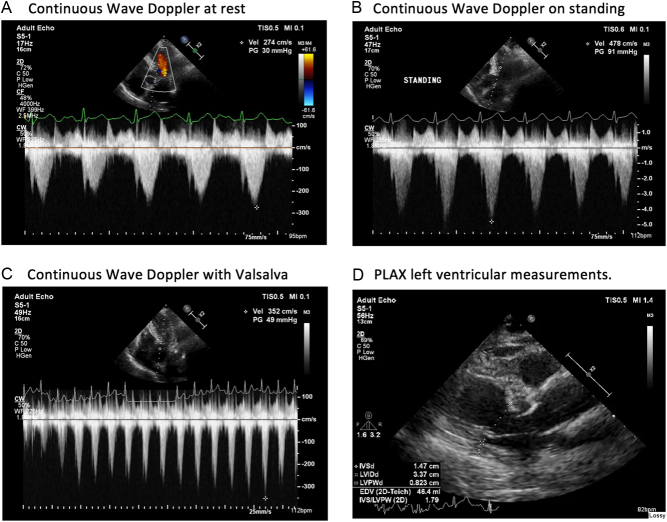
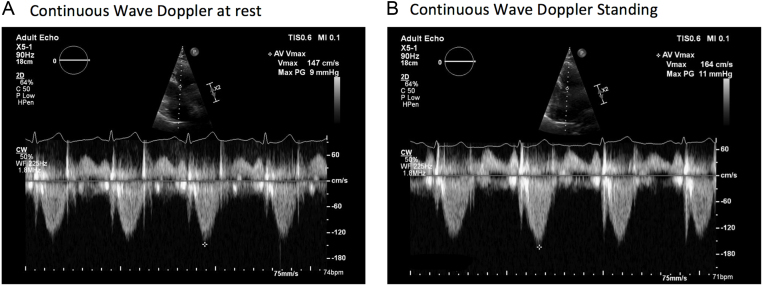
A 70-year-old female with exertional dyspnoea was found to have basal septal hypertrophy (BSH), or a 'basal septal bulge', with evidence of mild left ventricular outflow tract obstruction (LVOT) at rest on her initial echocardiogram. She was usually fit and well with no significant past medical history. She had no history of hypertension. She had never smoked. There was no family history of hypertrophic cardiomyopathy (HCM). A cardiac MRI did not demonstrate any typical features of HCM. ECG showed sinus tachycardia with a rate of 101 bpm but was otherwise unremarkable. She was referred for exercise echocardiography to assess for latent LVOT obstruction. Prior to commencing exercise, her LVOT gradient was re-assessed at rest. Her LVOT gradients were 30 mmHg at rest, 49 mmHg during Valsalva and 91 mmHg on standing. A diagnosis of significant latent LVOT obstruction was made and the patient was started on bisoprolol, a cardioselective beta-blocker. Bisoprolol was slowly uptitrated from 1.25 mg to 5 mg once daily, following which the patient reported a significant improvement in her symptoms with an improved exercise capacity. Follow-up echocardiography demonstrated a dramatic reduction in LVOT gradient, with a maximum of 11 mmHg assessed both with Valsalva and on standing. This case is a reminder that patients with a 'common' basal septal bulge can develop significant LVOT obstruction, the symptoms of which may respond to pharmacological therapy. Orthostatic assessment of LVOT gradient using echocardiography should be considered during standard LVOT obstruction provocation manoeuvres such as a Valsalva. Learning points: Differentiation between basal septal hypertrophy (BSH) and hypertrophic cardiomyopathy (HCM) may be challenging. Key factors favouring HCM include a positive family history of HCM or sudden cardiac death, septal thickness >15 mm/posterior wall thickness >11 mm, systolic anterior motion of the anterior mitral valve (SAM), late gadolinium enhancement on cardiac MRI, a causative genetic mutation associated with HCM and an abnormal ECG. Significant LVOT obstruction may develop in patients with BSH and is potentially responsive to pharmacotherapy. Standing reduces venous return, resulting in decreased LV volume. Compensatory mechanisms to maintain cardiac output involve sympathetic nervous system activation leading to increased LV contractility and subsequent increased LVOT gradient. Significant LVOT obstruction may be unmasked by an orthostatic posture. Orthostatic LVOT gradient assessment should be part of the routine echocardiographic assessment of all patients with an increased LVOT gradient at rest. The post-prandial state has been associated with increased LVOT gradient due to splanchnic dilatation and the consequent increased cardiac output required to maintain blood pressure. Post-prandial status should therefore be considered when assessing LVOT gradient.
Keywords: basal septal hypertrophy; latent LVOT obstruction; orthostatic LVOT assessment; provocable gradient.
Figures
Similar articles
-
Left Ventricular Outflow Tract Obstruction in Hypertrophic Cardiomyopathy Patients Without Severe Septal Hypertrophy: Implications of Mitral Valve and Papillary Muscle Abnormalities Assessed Using Cardiac Magnetic Resonance and Echocardiography.Circ Cardiovasc Imaging. 2015 Jul;8(7):e003132. doi: 10.1161/CIRCIMAGING.115.003132. Circ Cardiovasc Imaging. 2015. PMID: 26082555
-
Ischaemia as a cause of LVOT gradient reversal in HCM.Echo Res Pract. 2017 Dec;4(4):K31-K36. doi: 10.1530/ERP-17-0030. Epub 2017 Sep 4. Echo Res Pract. 2017. PMID: 28870983 Free PMC article.
-
Left ventricular outflow tract gradient provoked by upright position or exercise in treated patients with hypertrophic cardiomyopathy without obstruction at rest.Echocardiography. 2009 May;26(5):513-20. doi: 10.1111/j.1540-8175.2008.00851.x. Echocardiography. 2009. PMID: 19452607
-
Different mechanisms of mitral regurgitation in hypertrophic cardiomyopathy: A clinical case and literature review.Front Cardiovasc Med. 2022 Oct 28;9:1020054. doi: 10.3389/fcvm.2022.1020054. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36386345 Free PMC article. Review.
-
The evolution of basal septal hypertrophy: From benign and age-related normal variant to potentially obstructive and symptomatic cardiomyopathy.Echocardiography. 2017 Jul;34(7):1062-1072. doi: 10.1111/echo.13588. Epub 2017 Jun 8. Echocardiography. 2017. PMID: 28593726 Review.
Cited by
-
Interpretable machine learning for predicting isolated basal septal hypertrophy.PLoS One. 2025 Jun 30;20(6):e0325992. doi: 10.1371/journal.pone.0325992. eCollection 2025. PLoS One. 2025. PMID: 40587445 Free PMC article.
-
Use of Peripheral Nerve Blocks in Perioperative Management of Cases with Hypertrophic Cardiomyopathy Undergoing Lower Limb Orthopedic Surgeries.Anesth Essays Res. 2020 Apr-Jun;14(2):277-282. doi: 10.4103/aer.AER_48_20. Epub 2020 Oct 12. Anesth Essays Res. 2020. PMID: 33487829 Free PMC article.
References
-
- Authors/Task Force members, Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, et al 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). European Heart Journal 2014. 35 2733–2779. (10.1093/eurheartj/ehu284) - DOI - PubMed
-
- Critoph CH, Pantazis A, Tome Esteban MT, Salazar-Mendiguchía J, Pagourelias ED, Moon JC, Elliott PM. The influence of aortoseptal angulation on provocable left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Open Heart 2014. 1 1–8. (10.1136/openhrt-2014-000176) - DOI - PMC - PubMed
-
- Shah JS, Esteban T, Thaman R, Sharma R, Mist B, Pantazis A, Ward D, Kohli SK, Page SP, Demetrescu C, et al Prevalence of exercise induced left ventricular outflow tract obstruction in symptomatic patients with non-obstructive hypertrophic cardiomyopathy. Heart 2008. 94 1288–1294. (10.1136/hrt.2007.126003) - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
