

Modulation of temozolomide dose differentially affects T-cell response to immune checkpoint inhibition
- PMID: 30668768
- PMCID: PMC6556847
- DOI: 10.1093/neuonc/noz015
Modulation of temozolomide dose differentially affects T-cell response to immune checkpoint inhibition
Abstract
Background: The changes induced in host immunity and the tumor microenvironment by chemotherapy have been shown to impact immunotherapy response in both a positive and a negative fashion. Temozolomide is the most common chemotherapy used to treat glioblastoma (GBM) and has been shown to have variable effects on immune response to immunotherapy. Therefore, we aimed to determine the immune modulatory effects of temozolomide that would impact response to immune checkpoint inhibition in the treatment of experimental GBM.
Methods: Immune function and antitumor efficacy of immune checkpoint inhibition were tested after treatment with metronomic dose (MD) temozolomide (25 mg/kg × 10 days) or standard dose (SD) temozolomide (50 mg/kg × 5 days) in the GL261 and KR158 murine glioma models.
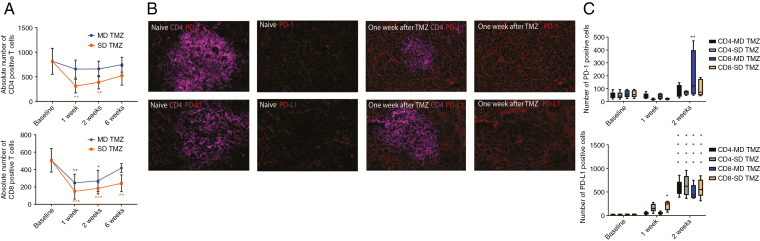
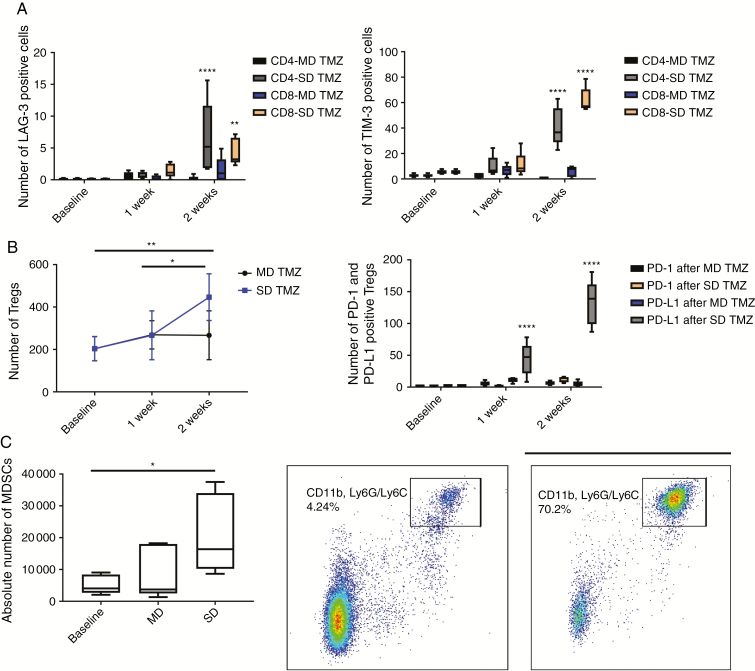
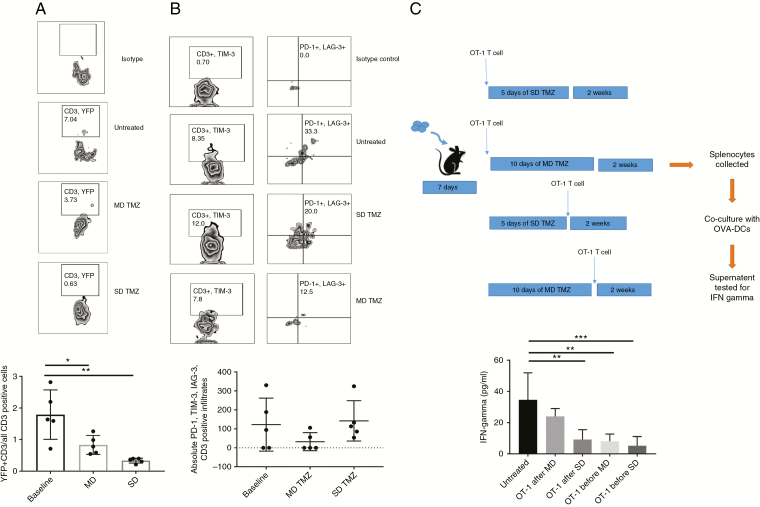
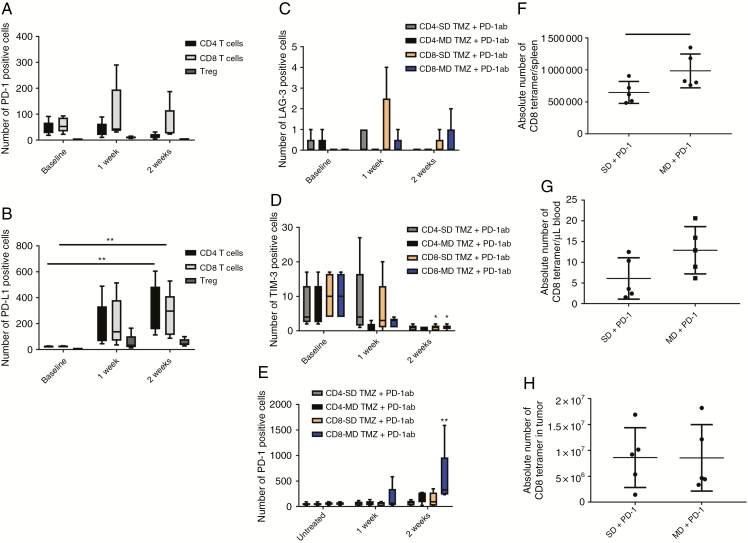
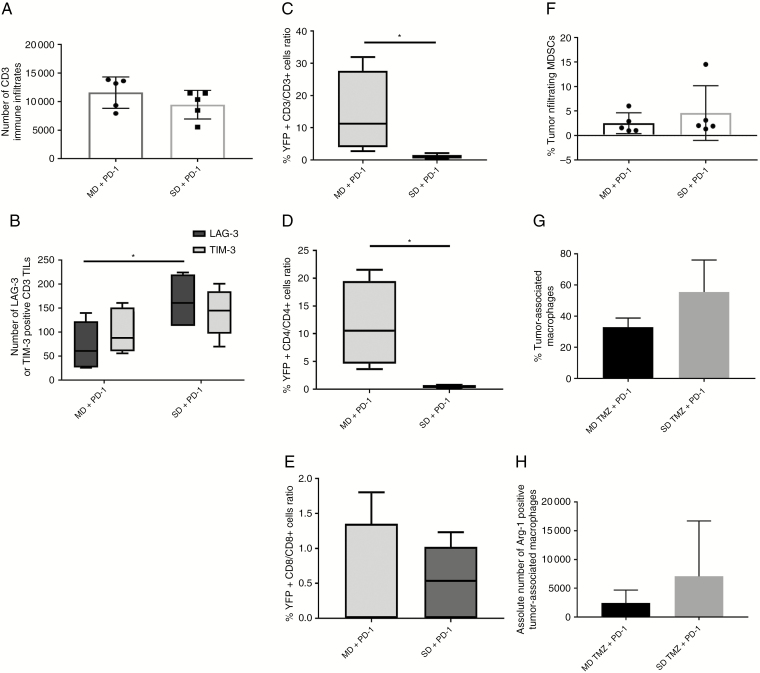
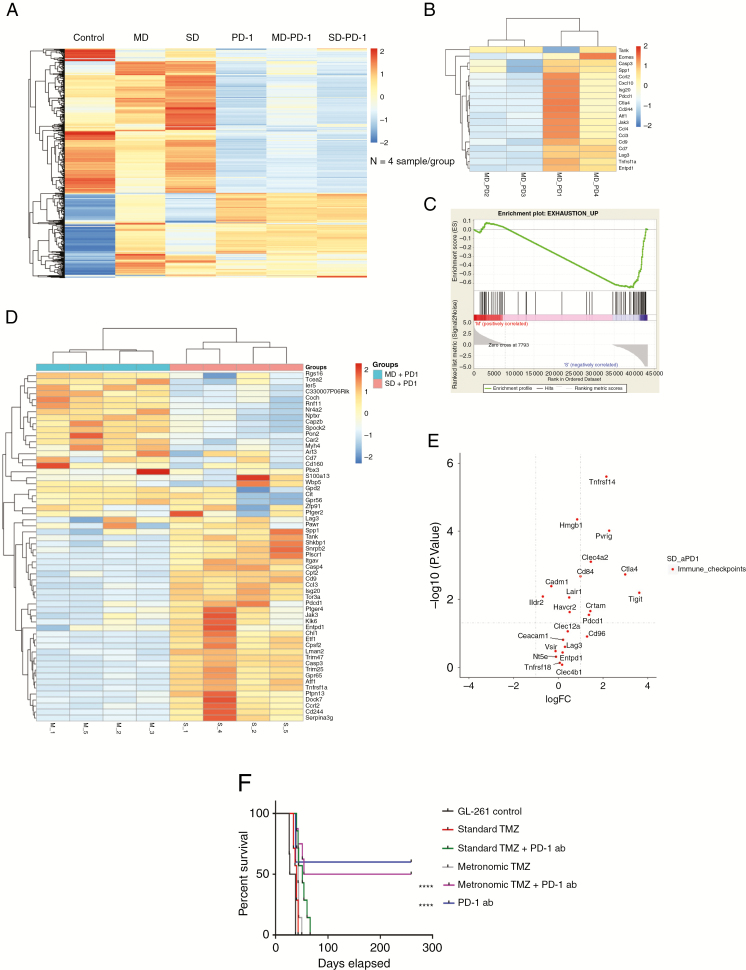
Results: SD temozolomide treatment resulted in an upregulation of markers of T-cell exhaustion such as LAG-3 and TIM-3 in lymphocytes which was not seen with MD temozolomide. When temozolomide treatment was combined with programmed cell death 1 (PD-1) antibody therapy, the MD temozolomide/PD-1 antibody group demonstrated a decrease in exhaustion markers in tumor infiltrating lymphocytes that was not observed in the SD temozolomide/PD-1 antibody group. Also, the survival advantage of PD-1 antibody therapy in a murine syngeneic intracranial glioma model was abrogated by adding SD temozolomide to treatment. However, when MD temozolomide was added to PD-1 inhibition, it preserved the survival benefit that was seen by PD-1 antibody therapy alone.
Conclusion: The peripheral and intratumoral immune microenvironments are distinctively affected by dose modulation of temozolomide.
Keywords: PD-1 antibody; glioblastoma; immune checkpoint inhibition; immunomodulation; temozolomide.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
How to integrate immunotherapy into standard of care in glioblastoma.Neuro Oncol. 2019 Jun 10;21(6):699-700. doi: 10.1093/neuonc/noz043. Neuro Oncol. 2019. PMID: 30938444 Free PMC article. No abstract available.
References
-
- Garon EB, Rizvi NA, Hui R, et al. ; KEYNOTE-001 Investigators Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372(21):2018–2028. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
