

'Need of the Hour': Early Diagnosis and Management of Multidrug Resistant Tuberculosis of the Spine: An Analysis of 30 Patients from a "High Multidrug Resistant Tuberculosis Burden" Country
- PMID: 30669824
- PMCID: PMC6454281
- DOI: 10.31616/asj.2018.0073
'Need of the Hour': Early Diagnosis and Management of Multidrug Resistant Tuberculosis of the Spine: An Analysis of 30 Patients from a "High Multidrug Resistant Tuberculosis Burden" Country
Abstract
Study design: Retrospective study.
Purpose: To report the prevalence of patients with multidrug-resistant (MDR) tubercular spondylodiscitis and their outcomes. Additionally, to assess the role of Xpert MTB/RIF assay in early detection of MDR tuberculosis.
Overview of literature: MDR tuberculosis is increasing globally. The World Health Organization (WHO) has strongly recommended Xpert MTB/RIF assay for early detection of tuberculosis.
Methods: From 2006 to 2015, a retrospective study was conducted on patients treated for MDR tuberculosis of the spine. Only patients whose diagnosis was confirmed using either culture and/or the Xpert MTB/RIF assay were included. Diagnostic method, treatment regimen, time taken to initiate second-line antituberculosis treatment (ATT), drug-related complications, and cost of medications were analyzed. All patients with MDR were treated according to the WHO recommendations for 2 years. The outcome parameters analyzed included clinical, biochemical, and radiological criteria to assess healing status.
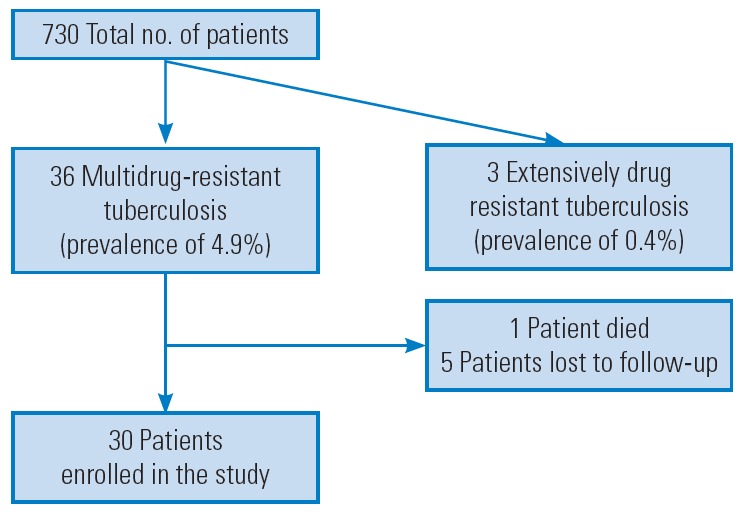
Results: From 2006 to 2015, a total of 730 patients were treated for tubercular spondylodiscitis. Of those, 36 had MDR tubercular spondylitis (prevalence, 4.9%), and three had extremely drug resistant tubercular spondylitis (prevalence, 0.4%). In this study, 30 patients, with a mean age of 29 years and a mean post-treatment follow-up of 24 months, were enrolled. The majority (77%) had secondary MDR, 17 (56%) underwent surgery, and 26 (87%) completed treatment for 2 years and were healed. Drug-related complications (33%) included ototoxicity, hypothyroidism, and hyperpigmentation of the skin. The average time taken for initiation of second line ATT for MDR patients with Xpert MTB/RIF assay as the diagnostic tool was 18 days, when compared to patients for whom the assay was not available which was 243 days.
Conclusions: The prevalence of MDR tubercular spondylodiscitis was 4.9%. In total, 87% of patients were healed with adequate treatment. The sensitivity and specificity of the Xpert MTB/RIF assay to detect MDR was 100% and 92.3%, respectively.
Keywords: Diagnosis; Multi drug resistance; Treatment; Tuberculosis.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- World Health Organization . Use of high burden country lists for TB by WHO in the post-2015 era [Internet] Geneva: World Health Organization; 2015. [cited 2017 Nov 24]. Available from: http://www.who.int/tb/publications/global_report/high_tb_burdencountryli....
-
- World Health Organization . Global tuberculosis report 2018 [Internet] Geneva: World Health Organization; 2018. [cited 2018 Nov 27]. Available from: http://www.who.int/tb/publications/global_report/en.
-
- World Health Organization . XpertMTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children: policy update. Geneva: World Health Organization; 2013. - PubMed
-
- Pawar UM, Kundnani V, Agashe V, Nene A, Nene A. Multidrug-resistant tuberculosis of the spine: is it the beginning of the end?: a study of twenty-five culture proven multidrug-resistant tuberculosis spine patients. Spine (Phila Pa 1976) 2009;34:E806–10. - PubMed
LinkOut - more resources
Full Text Sources
