

Profile and outcome of patients with emergency complications of renal failure presenting to an urban emergency department of a tertiary hospital in Tanzania
- PMID: 30669969
- PMCID: PMC6341653
- DOI: 10.1186/s12873-019-0229-2
Profile and outcome of patients with emergency complications of renal failure presenting to an urban emergency department of a tertiary hospital in Tanzania
Abstract
Background: Renal failure carries high mortality even in high-resource countries. Little attention has been paid to renal failure patients presenting acutely in emergency care settings in low-to-middle income countries (LMIC). Our aim was to describe the profile, management strategies and outcome of renal failure patients presenting with indications for emergent dialysis to an urban Emergency Department (ED) in a tertiary public hospital in Tanzania.
Methods: This was a prospective cohort study of consecutive patients (age ≥ 15 yrs) presenting to the Emergency Medicine Department of Muhimbili National Hospital from September 2017 to February 2018. All patients with renal failure and complications requiring acute dialysis were included. A structured data collection sheet was used to gather demographics, clinical presentation, management strategies and outcomes. Data were summarized with descriptive statistics. Logistic regressions were performed to determine factors associated with receiving dialysis and with mortality.
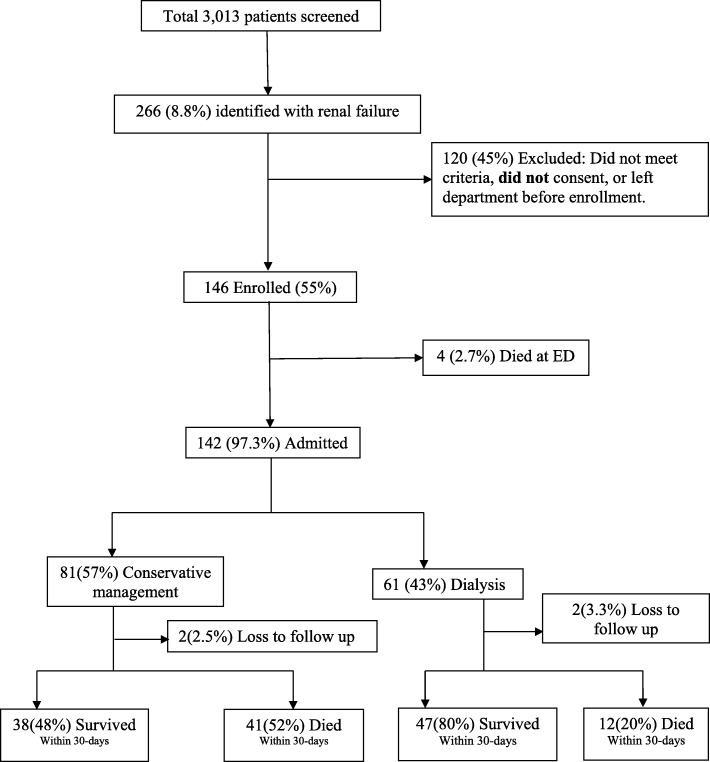
Results: We enrolled 146 patients, median age was 49 years (IQR 32-66 years), and 110 (75.3%) were male. Shortness of breath 67 (45.9%) and reduced urine output 58 (39.7%) were the most common presenting complaints. The most common complications were hyperkalemia 77 (53%), uremic encephalopathy 66 (45%) and pulmonary edema 54 (37%). All patients were hospitalized, and 61 (42%) received dialysis. Overall mortality was 39% (57 patients); the mortality in non-dialysed patients was 53% vs. 20% (p < 0.0005) in those receiving dialysis. 54% of patients with health insurance were dialyzed, compared to 39% who paid out of pocket (adjusted OR = 0.3, 95%CI: 0.1-0.9). Patients (≥55 years) were less likely to be dialysed (adjusted OR = 0.2 [0.1-0.9]). Independent predictors of mortality were vomiting (OR = 6.2, 95%CI: 1.8-22.2), oliguria (OR = 3.4, 95%CI: 1.2-9.5), pulmonary edema (OR = 4.6, 95%CI: 1.6-14.3), creatinine level > 1200umol/L (OR = 5.0 95%CI: 1.4-18.2), and not receiving dialysis (OR = 8.0, CI: 2.7-23.5). Female sex had a lower risk of dying (OR = 0.13, CI: 0.03-0.5).
Conclusions: In this ED in LIC, acute complications of renal failure created a need for ED stabilization and emergent dialysis. Overall in-hospital mortality was high; significantly higher in undialysed patients. Future studies in LICs should focus on identification of categories of patients that will do well with conservative therapy.
Keywords: Dialysis; Emergency complications; Emergency department; Renal failure.
Conflict of interest statement
Ethics approval and consent to participate
Permission to conduct the study was requested and granted from Muhimbili national hospital after review and approval by Institutional Review Board of Muhimbili University of Health and Allied Science (MUHAS). Written informed consent was sought from all patients, and child assent and parental permission sought prior to enrollment into the study.
Consent for publication
Not applicable.
Competing interests
The author
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Global Facts: About Kidney Disease [Internet]. The National Kidney Foundation. 2015 [cited 2017 Mar 21]. Available from: https://www.kidney.org/kidneydisease/global-facts-about-kidney-disease
