

Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: the first international randomized controlled trial for multimodal prehabilitation
- PMID: 30670009
- PMCID: PMC6341758
- DOI: 10.1186/s12885-018-5232-6
Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: the first international randomized controlled trial for multimodal prehabilitation
Abstract
Background: Colorectal cancer (CRC) is the second most prevalent type of cancer in the world. Surgery is the only curative option. However, postoperative complications occur in up to 50% of patients and are associated with higher morbidity and mortality rates, lower health related quality of life (HRQoL) and increased expenditure in health care. The number and severity of complications are closely related to preoperative functional capacity, nutritional state, psychological state, and smoking behavior. Traditional approaches have targeted the postoperative period for rehabilitation and lifestyle changes. However, recent evidence shows that the preoperative period might be the optimal moment for intervention. This study will determine the impact of multimodal prehabilitation on patients' functional capacity and postoperative complications.
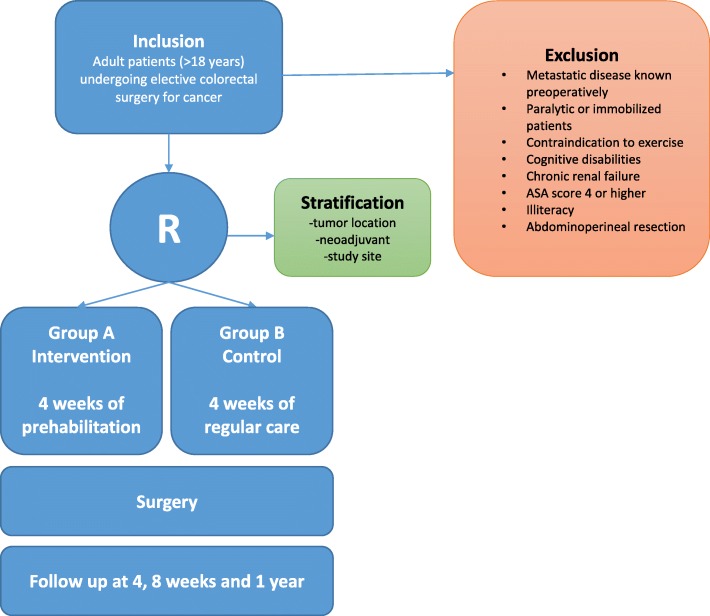
Methods/design: This international multicenter, prospective, randomized controlled trial will include 714 patients undergoing colorectal surgery for cancer. Patients will be allocated to the intervention group, which will receive 4 weeks of prehabilitation (group 1, prehab), or the control group, which will receive no prehabilitation (group 2, no prehab). Both groups will receive perioperative care in accordance with the enhanced recovery after surgery (ERAS) guidelines. The primary outcomes for measurement will be functional capacity (as assessed using the six-minute walk test (6MWT)) and postoperative status determined with the Comprehensive Complication Index (CCI). Secondary outcomes will include HRQoL, length of hospital stay (LOS) and a cost-effectiveness analysis.
Discussion: Multimodal prehabilitation is expected to enhance patients' functional capacity and to reduce postoperative complications. It may therefore result in increased survival and improved HRQoL. This is the first international multicenter study investigating multimodal prehabilitation for patients undergoing colorectal surgery for cancer.
Trial registration: Trial Registry: NTR5947 - date of registration: 1 August 2016.
Keywords: Colorectal cancer; Colorectal surgery; Comprehensive complication index; Enhanced recovery after surgery; Functional capacity; Postoperative complications; Prehabilitation.
Conflict of interest statement
Authors’ information
SJ is a PhD candidate in surgery and surgical oncology at Máxima Medical Center, Veldhoven, the Netherlands and at the NUTRIM School of Nutrition and Translational Research in Metabolism, Maastricht, The Netherlands.
FC is a Professor in anesthesiology at the Montréal General Hospital and McGill University, Montréal, Canada.
SD is a senior researcher at the Danish Cancer Society Research Center, Copenhagen, Denmark.
GT is a PhD candidate in surgery and surgical oncology at Máxima Medical Center, Veldhoven, the Netherlands.
RB is a PhD candidate and surgical resident at the Center for Surgical Science, Zealand University Hospital, Køge and Slagelse, Denmark.
MG is an anesthesiologist at Foch Hôpital, Paris, France.
NB is a sports physician at Foch Hôpital, Paris, France.
RA is a research coordinator and kinesiologist at the Montréal General Hospital, Montréal, Canada.
EM is a PhD candidate at the department of anesthesiology at the Montréal General Hospital, Montréal, Canada.
SB is a senior researcher at the Netherlands Comprehensive Cancer Organisation, Utrecht, the Netherlands.
GM is an anesthesiologist at the department of anesthesiology at the Hospital Clinic de Barcelona, IDIBAPS, University of Barcelona, Spain.
RL is a dietician at the department of nutrition at Máxima Medical Center, Veldhoven, the Netherlands.
CF is a Professor in surgery at the Ferrara University Hospital, Ferrara, Italy.
IG is a Professor in surgery at Center for Surgical Science, Zealand University Hospital, Køge and Roskilde, Denmark.
CJ is a Professor in research at the department of oncology at the Finsen Centre, Rigshospitalet and the Danish Cancer Society Research Center, Copenhagen, Denmark.
CS is a kinesiologist at the Montréal General Hospital and the McGill University, Montréal, Canada.
RR is a surgeon at Máxima Medical Center, Veldhoven, the Netherlands.
GS is a sports physician at Máxima Medical Center, Veldhoven, the Netherlands.
GDS is a surgeon at Máxima Medical Center, Veldhoven, the Netherlands.
Ethics approval and consent to participate
Medical ethical reviewing committee Máxima Medical Center number: NL58281.015.16. Ethical reviewing committees of all participating centers have additionally reviewed and approved the protocol. A written informed consent form for publication will be available for every study participant.
Consent for publication
Written informed consent has been obtained from all study participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global Cancer statistics, 2012. CA Cancer J Clin. 2015;65. - PubMed
-
- McDermott FD, Heeney A, Kelly ME, Steele RJ, Carlson GL, Winter DC. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg. 2015 Apr;102(5). - PubMed
-
- Govaert JA, Fiocco M, van Dijk WA, Scheffer AC, de Graaf EJ, Tollenaar RA, Wouters MW. Costs of complications after colorectal cancer surgery in the Netherlands. Building the business case for hospitals. Eur J Surg Oncol. 2015;41(8). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
