

A case of autonomous cortisol secretion in a patient with subclinical Cushing's syndrome, GNAS mutation, and paradoxical cortisol response to dexamethasone
- PMID: 30670014
- PMCID: PMC6343241
- DOI: 10.1186/s12902-019-0345-8
A case of autonomous cortisol secretion in a patient with subclinical Cushing's syndrome, GNAS mutation, and paradoxical cortisol response to dexamethasone
Abstract
Background: Increased urinary free cortisol in response to the oral administration of dexamethasone is a paradoxical reaction mainly reported in patients with primary pigmented nodular adrenocortical disease. Here, we describe the first case of subclinical Cushing's syndrome represented by autonomous cortisol secretion and paradoxical response to oral dexamethasone administration, harboring an activating mutation in the α subunit of the stimulatory G protein (GNAS).
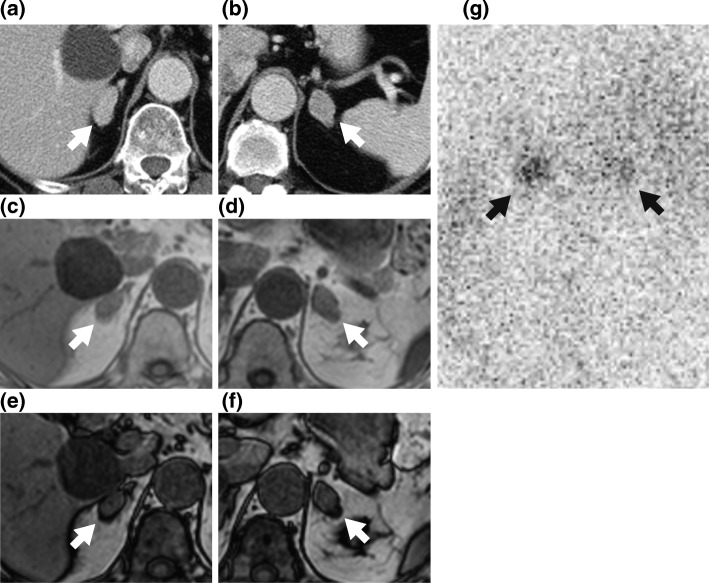
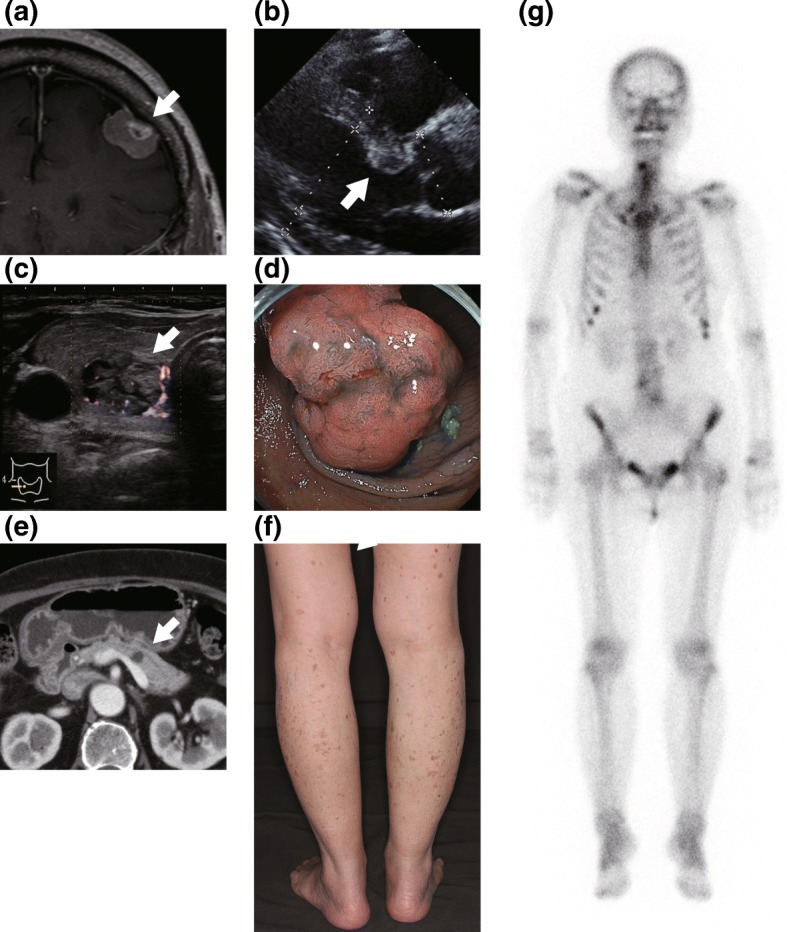
Case presentation: A 65-year-old woman was diagnosed with subclinical Cushing's syndrome during an evaluation for bilateral adrenal masses. Tumors of unknown origin were found in the heart, brain, thyroid gland, colon, pancreas, and both adrenal glands. Adenocarcinoma of the sigmoid colon and systemic brown-patchy skin pigmentation were also present. Her urinary cortisol levels increased in response to oral dexamethasone, while serum dehydroepiandrosterone-sulfate was not suppressed. After right adrenalectomy, genetic analysis of the resected tumor revealed the somatic GNAS activating mutation, p.R201H. Paradoxical urinary cortisol response persisted even after unilateral adrenal resection, although serum and urinary cortisol levels were attenuated.
Conclusions: This patient harbored a GNAS activating mutation, and presented with a mild cortisol- and androgen-producing adrenal adenoma. Administration of oral dexamethasone paradoxically increased cortisol levels, possibly via the stimulation of the cyclic adenosine monophosphate-dependent protein kinase A signaling pathway, which is seen in patients with pigmented nodular adrenocortical disease or Carney complex. GNAS mutations may provide clues to the mechanisms of hyper-function and tumorigenesis in the adrenal cortex, especially in bilateral adrenal masses accompanied by multiple systemic tumors. Examining GNAS mutations could help physicians detect extra-adrenal malignancies, which may contribute to an improved prognosis for patients with this type of Cushing's syndrome.
Keywords: Adrenal tumor; Cortisol; Cushing’s syndrome; Cyclic-AMP; GNAS; Protein kinase A.
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in this study were in accordance with the ethical standards of the Institutional Review Board of Kyushu university hospital and with the principles of the Declaration of Helsinki 2013. The patient provided informed consent, and approval by an ethics review board were exempted by the Institutional Review Board of Kyushu university hospital for this case report.
Consent for publication
Written informed consent for publication of the patient’s clinical details and clinical images was obtained from the patient.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
ACTH-independent Cushing's syndrome due to ectopic endocrinologically functional adrenal tissue caused by a GNAS heterozygous mutation: a rare case of McCune-Albright syndrome accompanied by central amenorrhea and hypothyroidism: a case report and literature review.Front Endocrinol (Lausanne). 2022 Jul 25;13:934748. doi: 10.3389/fendo.2022.934748. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35966069 Free PMC article. Review.
-
Clinical characteristics of PRKACA mutations in Chinese patients with adrenal lesions: a single-centre study.Clin Endocrinol (Oxf). 2016 Dec;85(6):954-961. doi: 10.1111/cen.13134. Epub 2016 Jul 27. Clin Endocrinol (Oxf). 2016. PMID: 27296931
-
Cushing's syndrome due to bilateral adrenocortical adenomas with unique histological features.Endocr J. 2003 Apr;50(2):155-62. doi: 10.1507/endocrj.50.155. Endocr J. 2003. PMID: 12803235
-
GNAS mutations in adrenal aldosterone-producing adenomas.Endocr J. 2016;63(2):199-204. doi: 10.1507/endocrj.EJ15-0642. Epub 2016 Jan 6. Endocr J. 2016. PMID: 26743443
-
Subclinical Cushing's syndrome.Endocrinol Metab Clin North Am. 2000 Mar;29(1):43-56. doi: 10.1016/s0889-8529(05)70115-8. Endocrinol Metab Clin North Am. 2000. PMID: 10732263 Review.
Cited by
-
An Overlooked Disease: Minimal Autonomous Cortisol Secretion (MACS). A Narrative Review.Endocr Metab Immune Disord Drug Targets. 2024;24(13):1518-1524. doi: 10.2174/0118715303266569231129101847. Endocr Metab Immune Disord Drug Targets. 2024. PMID: 38686896 Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
