

Unstable Genome and Transcriptome Dynamics during Tumor Metastasis Contribute to Therapeutic Heterogeneity in Colorectal Cancers
- PMID: 30670495
- PMCID: PMC7875093
- DOI: 10.1158/1078-0432.CCR-18-3460
Unstable Genome and Transcriptome Dynamics during Tumor Metastasis Contribute to Therapeutic Heterogeneity in Colorectal Cancers
Abstract
Purpose: Genomic and transcriptomic alterations during metastasis are considered to affect clinical outcome of colorectal cancers, but detailed clinical implications of metastatic alterations are not fully uncovered. We aimed to investigate the effect of metastatic evolution on in vivo treatment outcome, and identify genomic and transcriptomic alterations associated with drug responsiveness.
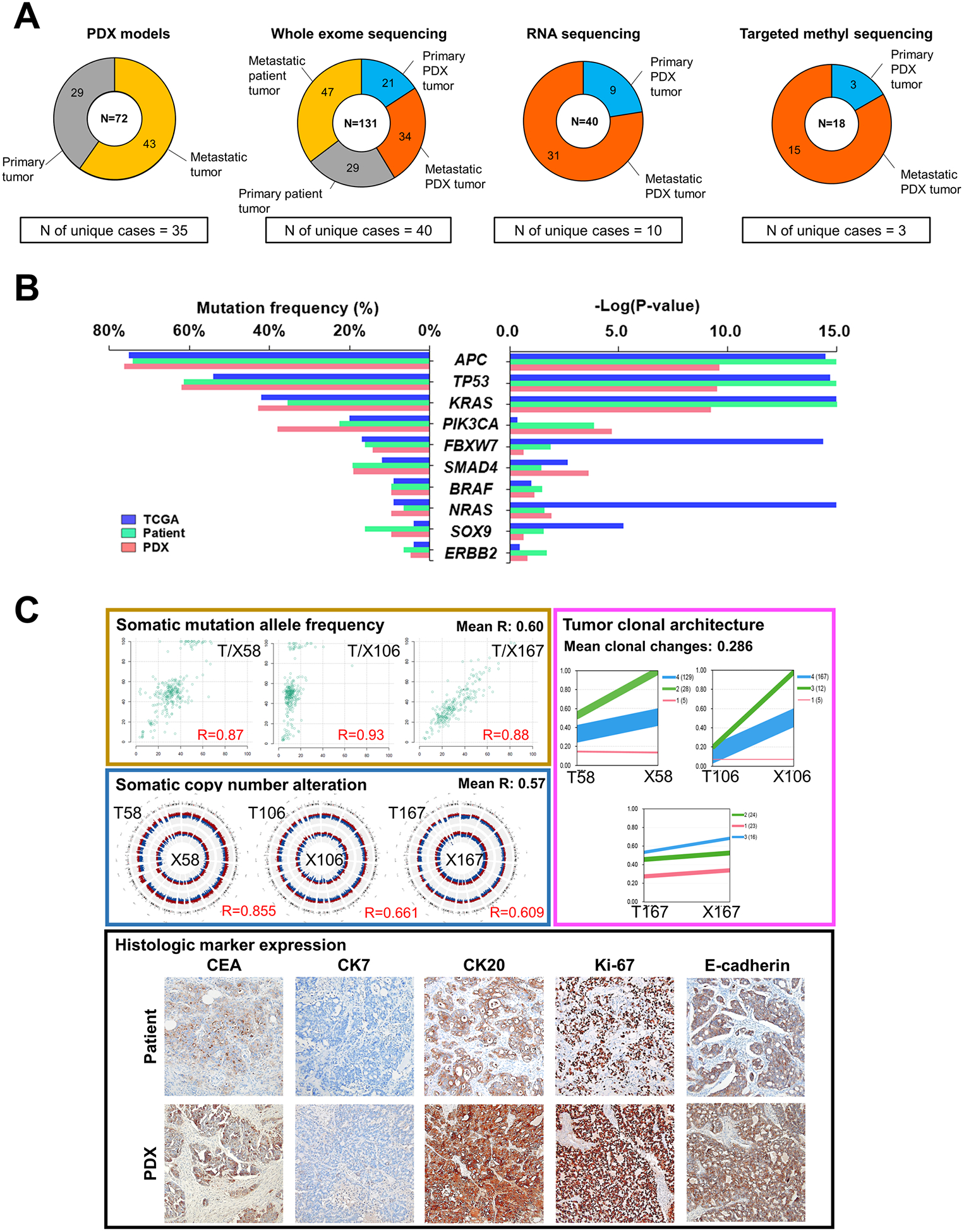
Experimental design: We developed and analyzed patient-derived xenograft (PDX) models from 35 patients with colorectal cancer including 5 patients with multiple organ metastases (MOMs). We performed whole-exome, DNA methylation, and RNA sequencing for patient and PDX tumors. With samples from patients with MOMs, we conducted phylogenetic and subclonal analysis and in vivo drug efficacy test on the corresponding PDX models.
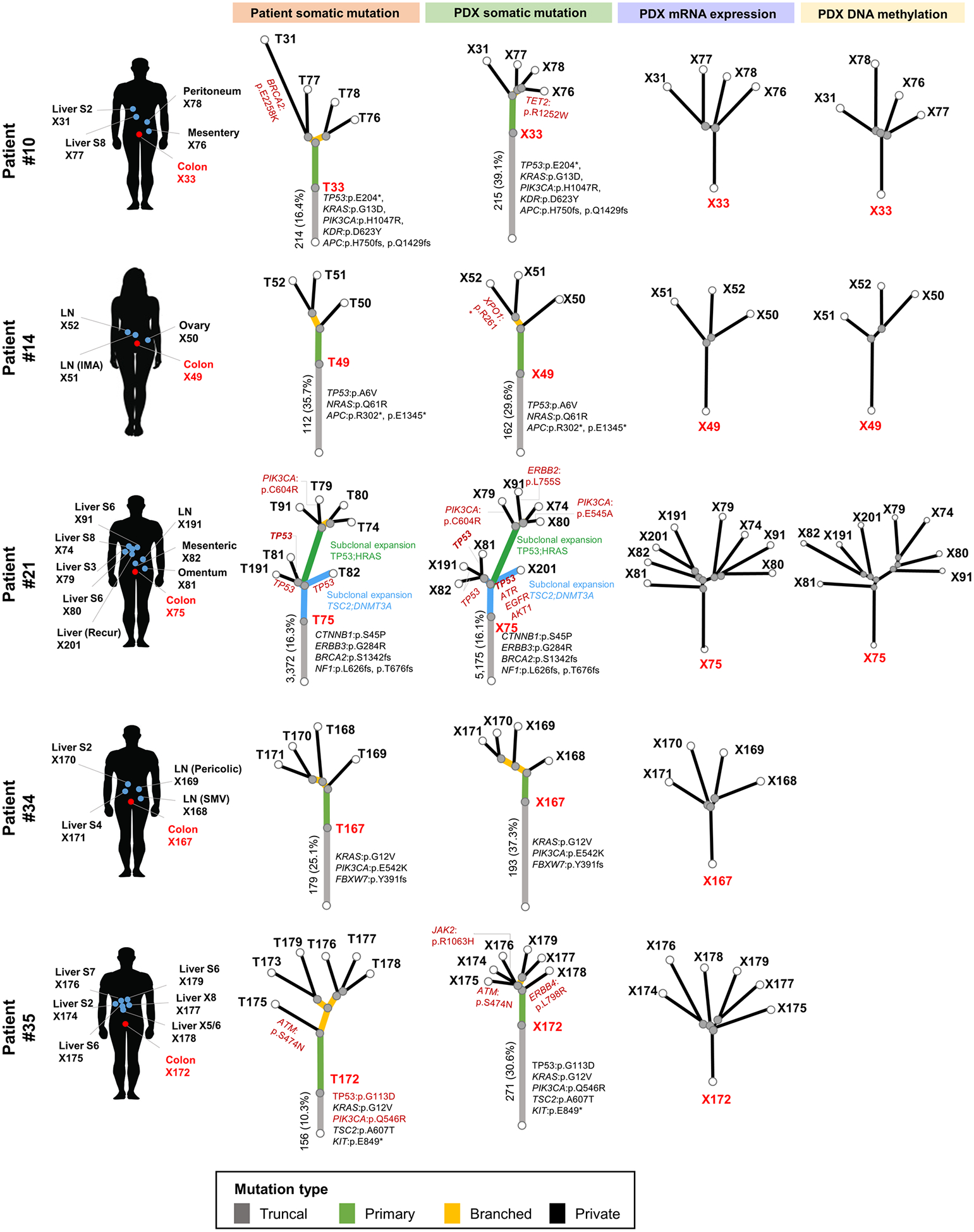
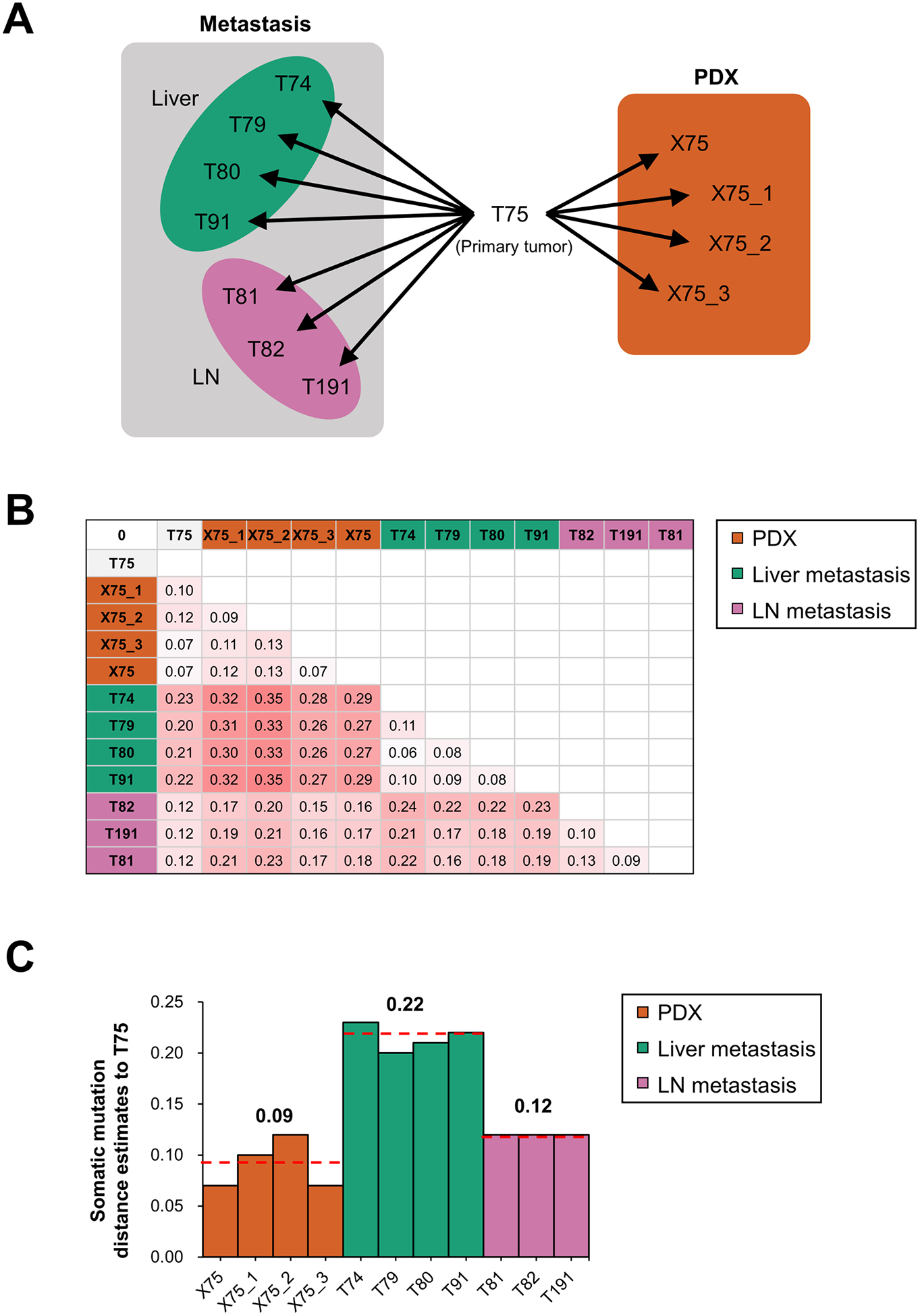
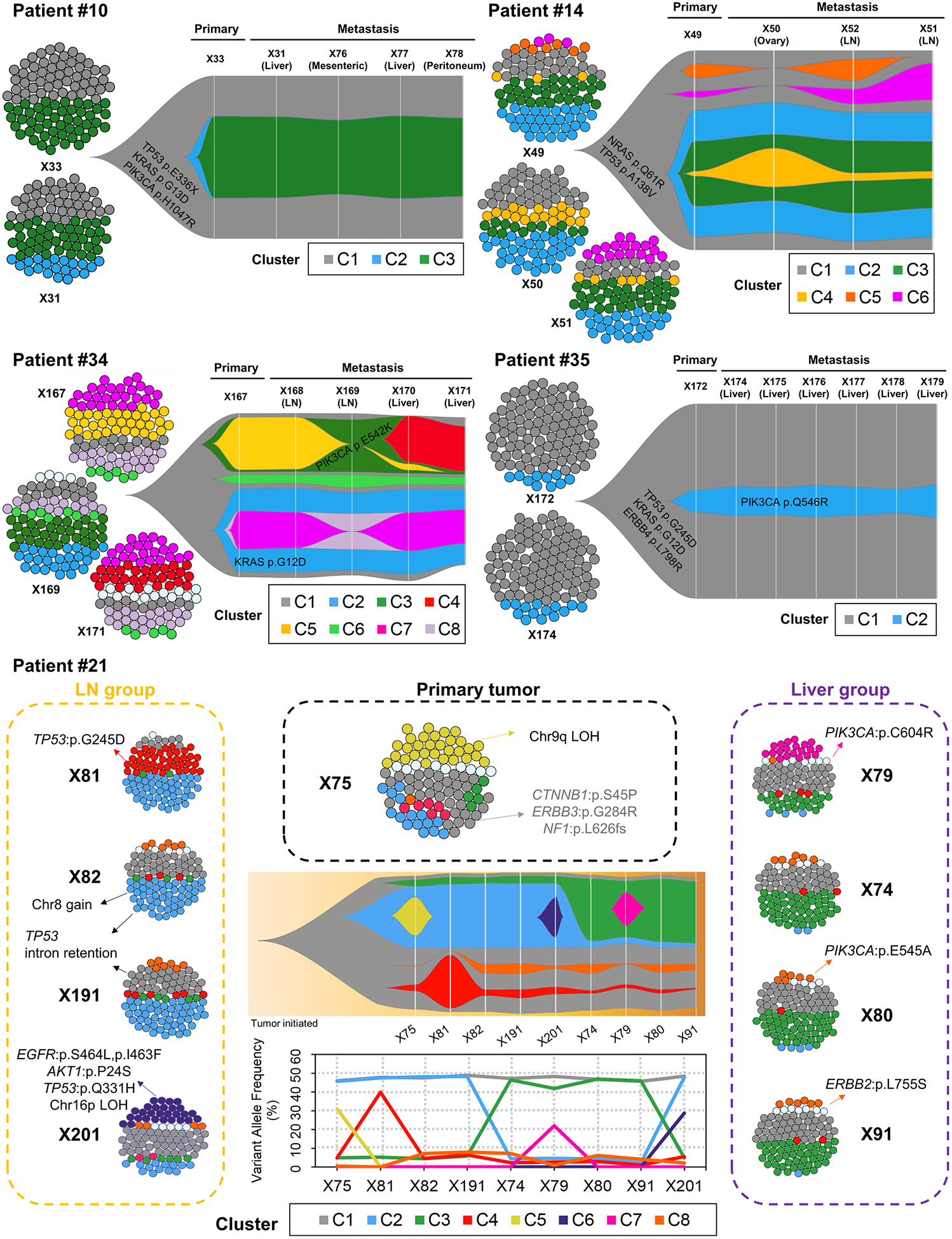
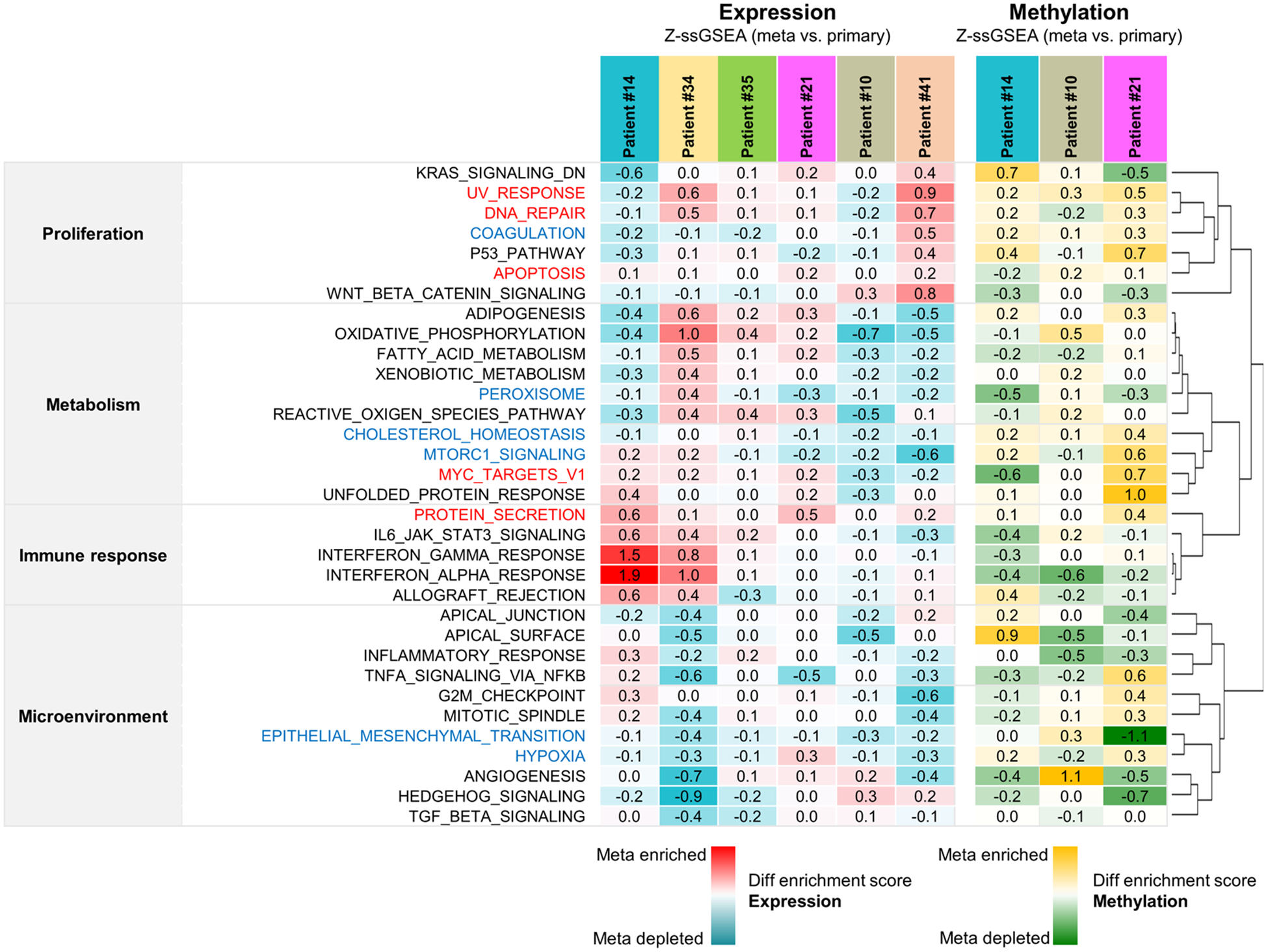
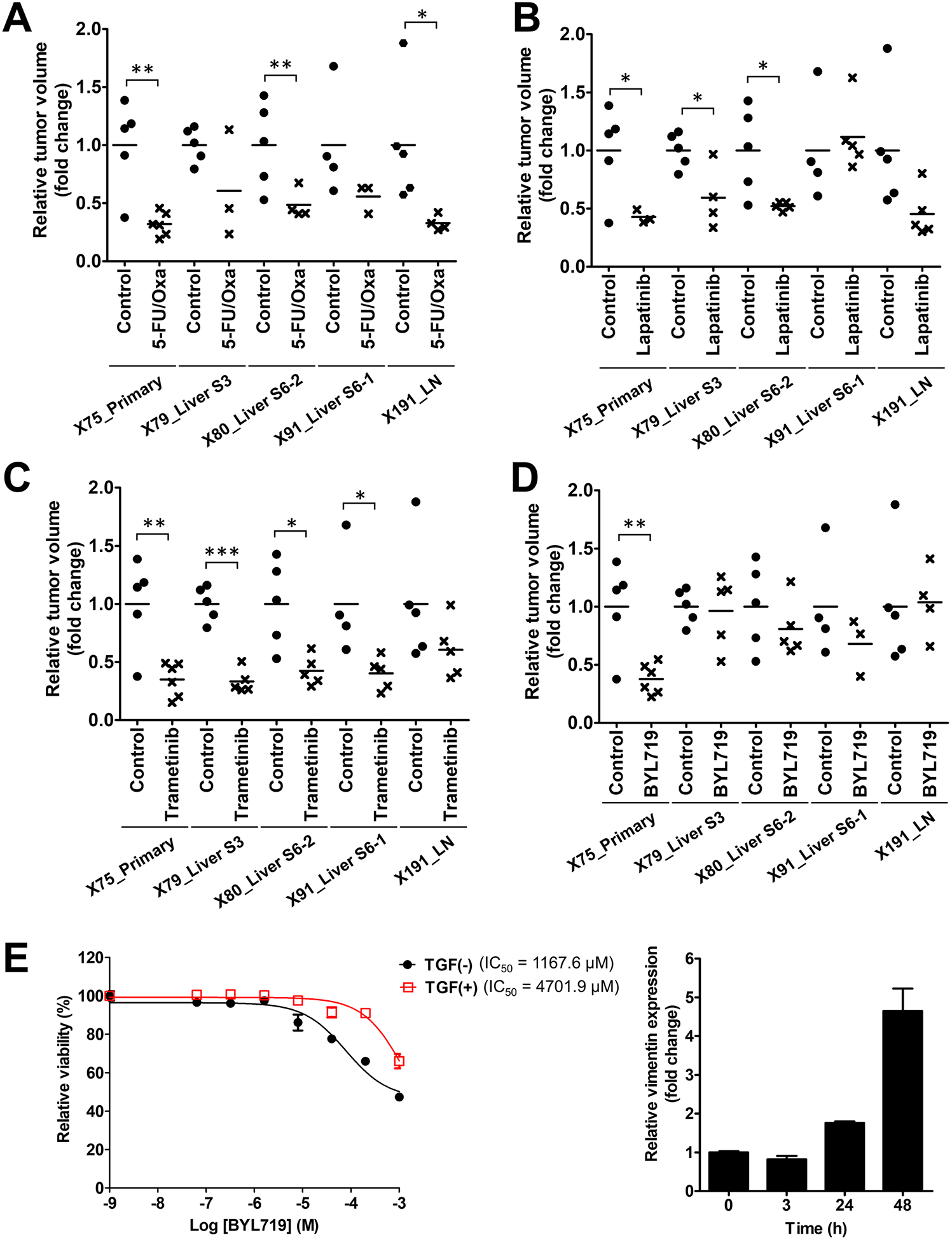
Results: Phylogenetic analysis using mutation, expression, and DNA methylation data in patients with MOMs showed that mutational alterations were closely connected with transcriptomic and epigenomic changes during the tumor evolution. Subclonal analysis revealed that initial primary tumors with larger number of subclones exhibited more dynamic changes in subclonal architecture according to metastasis, and loco-regional and distant metastases occurred in a parallel or independent fashion. The PDX models from MOMs demonstrated therapeutic heterogeneity for targeted treatment, due to subclonal acquisition of additional mutations or transcriptomic activation of bypass signaling pathway during tumor evolution.
Conclusions: This study demonstrated in vivo therapeutic heterogeneity of colorectal cancers using PDX models, and suggests that acquired subclonal alterations in mutations or gene expression profiles during tumor metastatic processes can be associated with the development of drug resistance and therapeutic heterogeneity of colorectal cancers.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
