

Prognosis of relapse after hematopoietic cell transplant (HCT) for treatment of leukemia or myelodysplastic syndrome (MDS) in children
- PMID: 30670822
- PMCID: PMC6646113
- DOI: 10.1038/s41409-019-0438-z
Prognosis of relapse after hematopoietic cell transplant (HCT) for treatment of leukemia or myelodysplastic syndrome (MDS) in children
Abstract
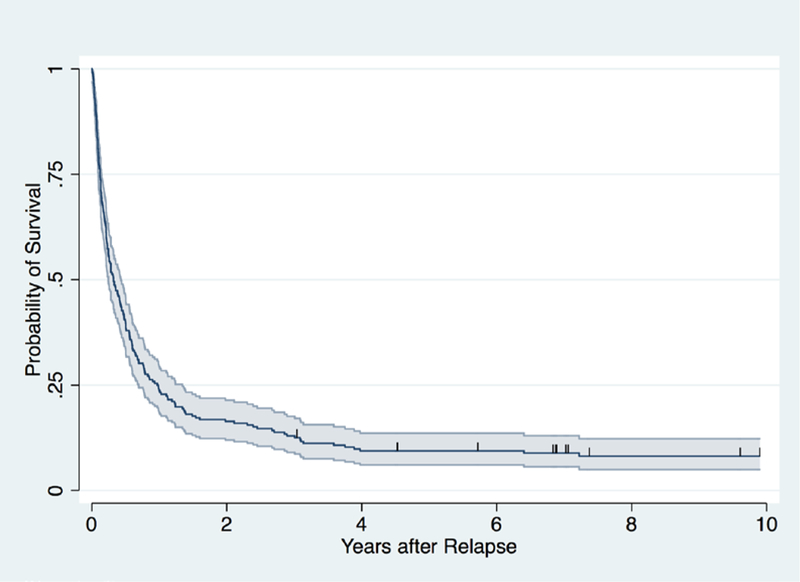
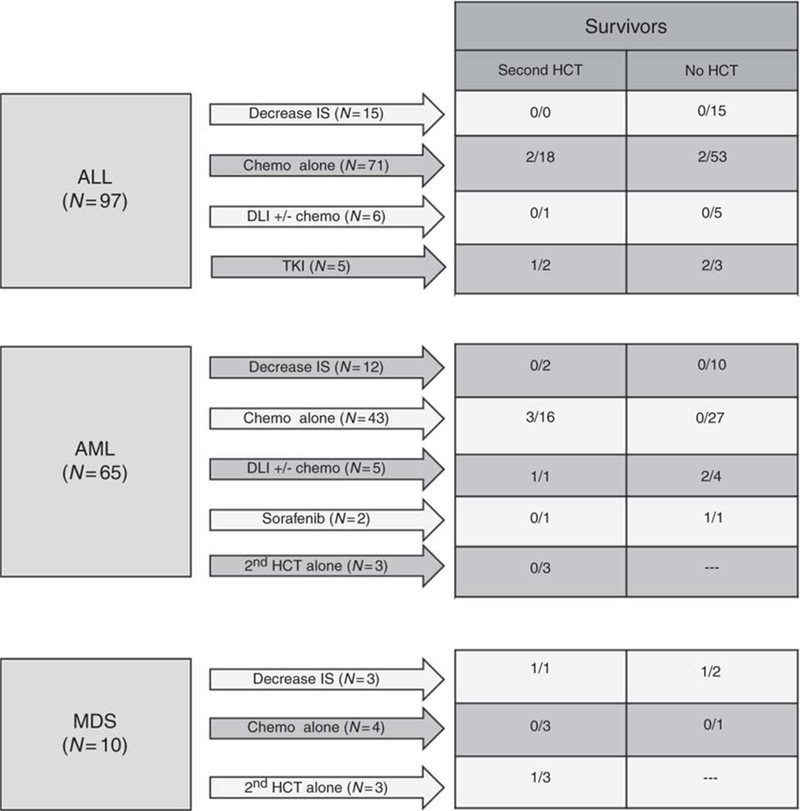
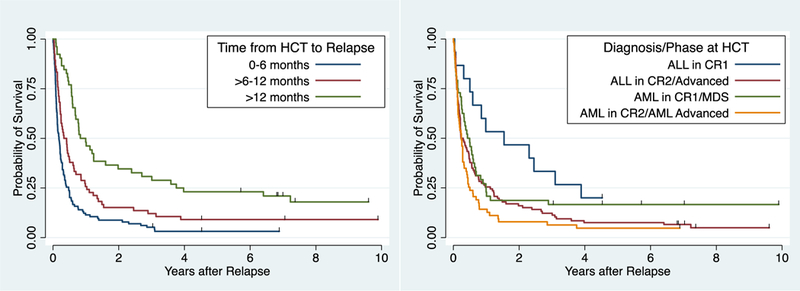
We studied 232 consecutive children transplanted between 1990 and 2011 with relapse after first hematopoietic cell transplant (HCT). Kaplan-Meier survival and hazard ratios for mortality were calculated for factors known at time of relapse using Cox proportional hazards models. The median (range) age at time of first HCT was 10.9 (0.5-20.9) years, time to relapse was 6.1 (0.2-89.5) months after HCT, and age at relapse was 11.7 (0.7-23.6) years. The 3-year overall survival (OS) after relapse was 13% (95% confidence interval (CI): 9%, 18%).The median (range) follow-up for the 18 surviving patients was 7.2 (3.0-24.4) years after relapse. The remaining 214 died after a median of 3 months (0.02-190.4). OS was not significantly different for patients with ALL as compared to AML. Fifty-one patients proceeded to second transplant of whom nine survive. Factors associated with improved survival included late relapse (>12 months), ALL in first CR at the time of first transplant and chemotherapy-based first conditioning regimens. These results can be used to counsel patients at the time of relapse after first transplant and as a baseline for comparison as to the effectiveness of newer therapies which are greatly needed for treatment of post-transplant relapse.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Shiba N, Ohki K, Kobayashi T, et al. High PRDM16 expression identifies a prognostic subgroup of pediatric acute myeloid leukaemia correlated to FLT3-ITD, KMT2A-PTD, and NUP98-NSD1: the results of the Japanese Paediatric Leukaemia/Lymphoma Study Group AML-05 trial. Br J Haematol. 2016;172:581–591. - PubMed
-
- Borowitz MJ, Shuster J, Carroll AJ, et al. Prognostic significance of fluorescence intensity of surface marker expression in childhood B-precursor acute lymphoblastic leukemia. Blood. 1997;89:3960–3966. - PubMed
-
- Roberts KG, Mullighan CG. Genomics in acute lymphoblastic leukaemia: insights and treatment implications. Nat Rev Clin Oncol. 2015;12:344–357. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
