

A Retrospective Analysis of Prolonged Empiric Antibiotic Therapy for Pneumonia Among Adult Neurocritical Care Patients
- PMID: 30671159
- PMCID: PMC6327239
- DOI: 10.1177/1941874418792138
A Retrospective Analysis of Prolonged Empiric Antibiotic Therapy for Pneumonia Among Adult Neurocritical Care Patients
Abstract
Background and purpose: Current literature reports that half of critically ill patients are continued on broad-spectrum antibiotics beyond 72 hours despite no confirmed infection. The purpose of this retrospective study was to identify the incidence of and risk factors for prolonged empiric antimicrobial therapy (PEAT) in adult neurocritical care (NCC) patients treated for pneumonia, hypothesizing that NCC patients will have a higher incidence of PEAT.
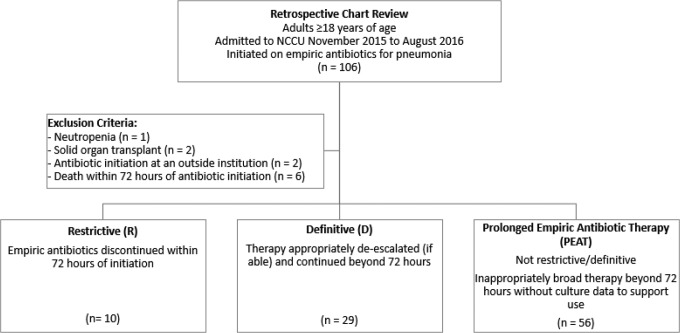
Methods: This is a retrospective chart review of adult NCC patients treated for pneumonia. Antibiotic therapy was classified as restrictive, definitive, or PEAT based on culture results and timing of discontinuation or de-escalation.
Results: A total of 95 patients (median age: 57 years; 28.4% female; admission diagnosis: 73.7% cerebrovascular, 10.5% neuromuscular, and 15.8% seizure-related) were included in this study. Overall, 59% of antibiotic regimens were considered PEAT, with vancomycin and piperacillin/tazobactam being most commonly prescribed. Median duration of therapy was 6.8 days, with shorter duration in patients with negative culture results compared to those with positive culture results (6.1 days [interquartile range, IQR 4.0-8.3] vs 7.2 days [IQR 5.8-10.3], P < .05). On multivariable analysis, elevated baseline white blood cell count, meeting Centers for Disease Control criteria for pneumonia, and negative bacterial culture were significantly associated with PEAT.
Conclusion: The incidence of prolonged empiric antibiotic use was high in the NCC population. Patients are at particular risk for PEAT if they have negative cultures. All but one patient did not meet criteria for central fever, highlighting the challenges in identifying fever etiology in the NCC population.
Keywords: critical illness; culture negative; neurocritical care; pneumonia; prolonged empiric antibiotic therapy.
Conflict of interest statement
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Frequency of empiric antibiotic de-escalation in an acute care hospital with an established Antimicrobial Stewardship Program.BMC Infect Dis. 2016 Dec 12;16(1):751. doi: 10.1186/s12879-016-2080-3. BMC Infect Dis. 2016. PMID: 27955625 Free PMC article.
-
A Multicenter Evaluation of Prolonged Empiric Antibiotic Therapy in Adult ICUs in the United States.Crit Care Med. 2015 Dec;43(12):2527-34. doi: 10.1097/CCM.0000000000001294. Crit Care Med. 2015. PMID: 26457751
-
Empiric broad-spectrum antibiotic therapy of nosocomial pneumonia in the intensive care unit: a prospective observational study.Crit Care. 2006;10(3):R78. doi: 10.1186/cc4919. Epub 2006 May 16. Crit Care. 2006. PMID: 16704742 Free PMC article.
-
Evaluation of empiric antibiotic de-escalation in febrile neutropenia.J Oncol Pharm Pract. 2016 Oct;22(5):696-701. doi: 10.1177/1078155215597558. Epub 2015 Jul 30. J Oncol Pharm Pract. 2016. PMID: 26227319 Review.
-
Considerations in the choice and administration of agents for empiric antimicrobial therapy.Surg Infect (Larchmt). 2005;6 Suppl 2:S-71-82. Surg Infect (Larchmt). 2005. PMID: 23577498 Review.
Cited by
-
Understanding healthcare provider preferences for ordering respiratory cultures to diagnose ventilator associated pneumonia: A discrete choice experiment.Antimicrob Steward Healthc Epidemiol. 2022 Jul 15;2(1):e120. doi: 10.1017/ash.2022.267. eCollection 2022. Antimicrob Steward Healthc Epidemiol. 2022. PMID: 36483413 Free PMC article.
-
Application of Real-Time PCR Syndromic Panel on Lower Respiratory Tract Samples: Potential Use for Antimicrobial De-Escalation.Microorganisms. 2025 Jul 16;13(7):1678. doi: 10.3390/microorganisms13071678. Microorganisms. 2025. PMID: 40732186 Free PMC article.
References
-
- O’Horo JC, Sampathkumar P. Infections in neurocritical care. Neurocrit Care. 2017;27(3):458–467. - PubMed
-
- Hocker SE, Tian L, Li G, Steckelberg JM, Mandrekar JN, Rabinstein AA. Indicators of central fever in the neurologic intensive care unit. JAMA Neurol. 2013;70(12):1499–1504. - PubMed
-
- Dettenkofer M, Ebner W, Els T, et al. Surveillance of nosocomial infections in a neurology intensive care unit. J Neurol. 2001;248(11):959–964. - PubMed
-
- American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. - PubMed
LinkOut - more resources
Full Text Sources