The analgesic efficacy of the continuous adductor canal block compared to continuous intravenous fentanyl infusion with a single-shot adductor canal block in total knee arthroplasty: a randomized controlled trial
- PMID: 30671201
- PMCID: PMC6333576
- DOI: 10.3344/kjp.2019.32.1.30
The analgesic efficacy of the continuous adductor canal block compared to continuous intravenous fentanyl infusion with a single-shot adductor canal block in total knee arthroplasty: a randomized controlled trial
Abstract
Background: The adductor canal block (ACB) is an effective intervention for postoperative analgesia following total knee arthroplasty (TKA). However, the ideal ACB regimen has not yet been established. We compared the analgesic effects between a continuous ACB group and fentanyl-based intravenous patient-controlled analgesia (IV-PCA) with a single-shot ACB group.
Methods: Patients who underwent TKA were randomly allocated to either a continuous ACB group (Group CACB) or IV-PCA with a single-shot ACB group (Group IVACB). Before the surgery, ultrasound guided ACB with 0.5% ropivacaine 20 cc was provided to all patients. Before skin incision, the infusion system (0.2% ropivacaine through an adductor canal catheter in group CACB vs. intravenous fentanyl in group IVACB) was connected. The postoperative pain severity; the side effects of local anesthetics and opioids; administration of rescue analgesics and anti-emetics; and sensorimotor deficits were measured.
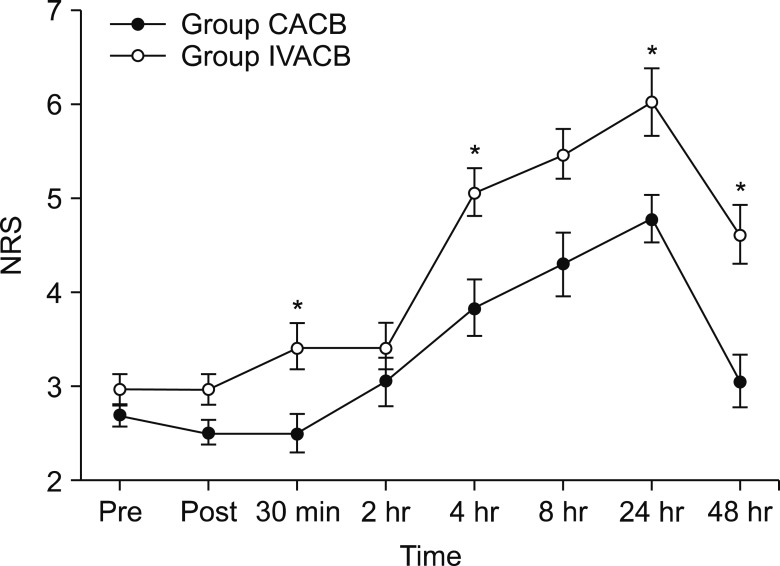
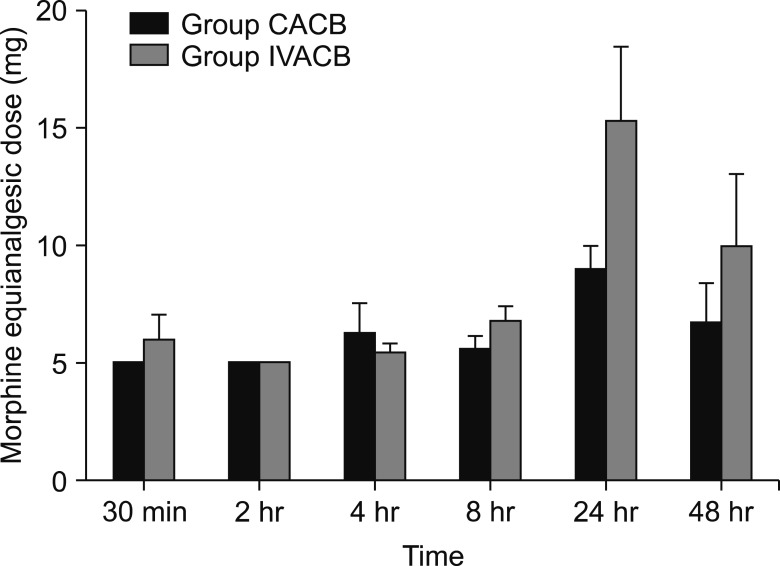
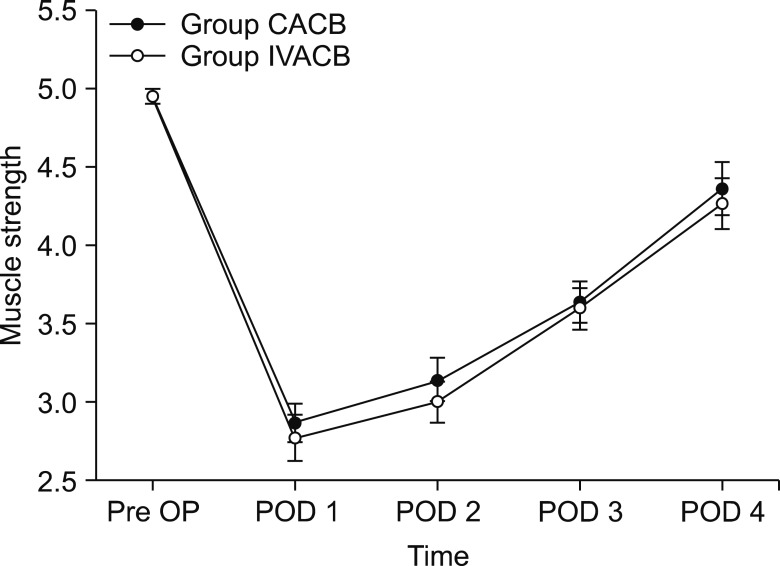
Results: Postoperative pain severity was significantly higher in the IVACB group at 30 min, 4 h, 24 h, and 48 h after surgery. The averages and standard deviations (SD) of the NRS score of postoperative pain were 0.14 ± 0.37, 4.57 ± 2.37, 6.00 ± 1.63, and 4.28 ± 1.49, respectively in the IVACB group. Rescue analgesic requirements and quadriceps muscle strength were not statistically different between the groups throughout the postoperative period. Moreover, rescue antiemetic requirements were higher in group IVACB than group CACB.
Conclusions: In this study, the continuous ACB provided superior analgesia and fewer side effects without any significant motor deficit than the IV-PCA with a single-shot ACB.
Keywords: Analgesia; Fentanyl; Knee replacement arthroplasty; Local anesthetics; Nausea; Opioid; Pain management; Patient controlled analgesia; Postoperative pain; Ropivacaine; Vomiting.
Conflict of interest statement
CONFLICT OF INTEREST: The authors declare that they have no conflict of interest.
Figures
References
-
- Fischer HB, Simanski CJ, Sharp C, Bonnet F, Camu F, Neugebauer EA, et al. A procedure-specific systematic review and consensus recommend ations for postoperative analgesia following total knee arthroplasty. Anaesthesia. 2008;63:1105–1123. - PubMed
-
- Chung MY, Kim CJ. The effect of bilateral femoral nerve block combined with intravenous patient-controlled analgesia after a bilateral total knee replacement. Korean J Pain. 2008;21:211–216.
-
- Jæger P, Zaric D, Fomsgaard JS, Hilsted KL, Bjerregaard J, Gyrn J, et al. Add uctor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. 2013;38:526–532. - PubMed
LinkOut - more resources
Full Text Sources