

Long-Term Endocrine and Exocrine Insufficiency After Pancreatectomy
- PMID: 30671791
- PMCID: PMC6646099
- DOI: 10.1007/s11605-018-04084-x
Long-Term Endocrine and Exocrine Insufficiency After Pancreatectomy
Abstract
Purpose: To identify peri-operative risk factors and time to onset of pancreatic endocrine/exocrine insufficiency.
Methods: We retrospectively analyzed a single institutional series of patients who underwent pancreaticoduodenectomy (PD) or distal pancreatectomy (DP) between 2000 and 2015. Endocrine/exocrine insufficiencies were defined as need for new pharmacologic intervention. Cox proportional modeling was used to identify peri-operative variables to determine their impact on post-operative pancreatic insufficiency.
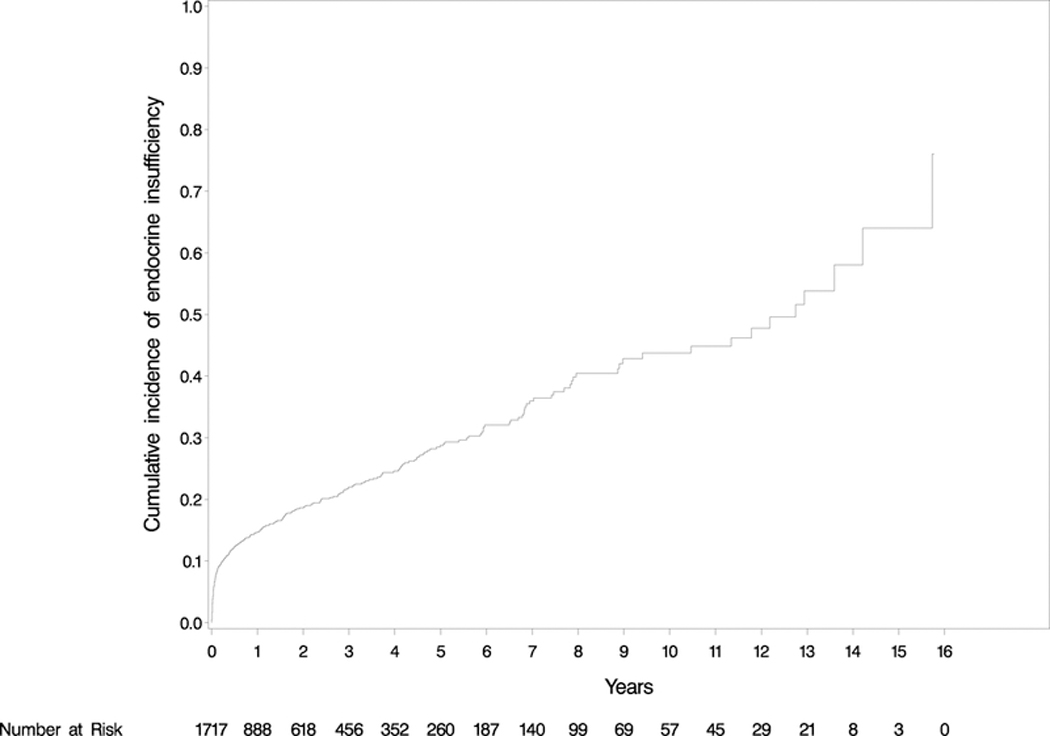
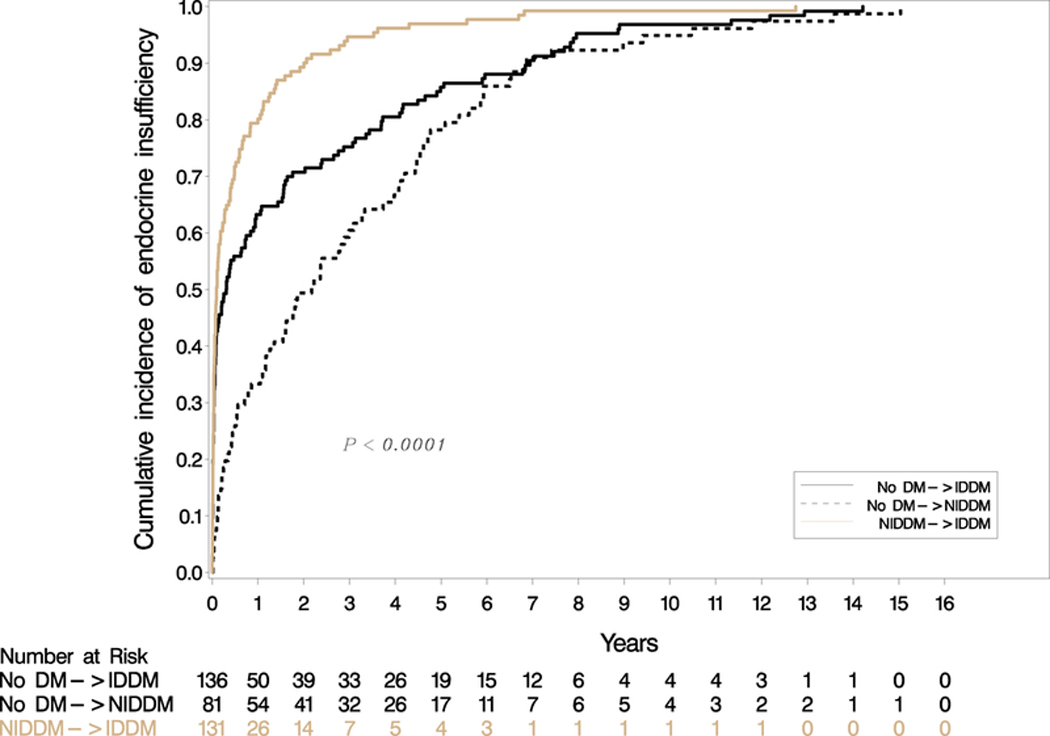
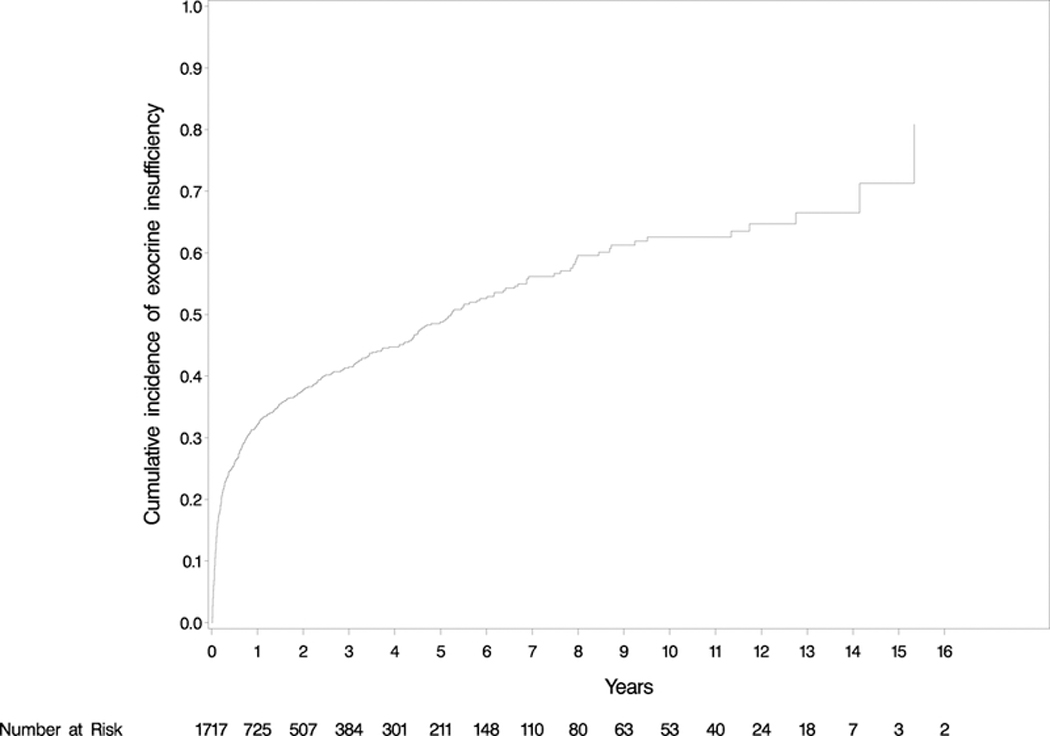
Results: A total of 1717 patient records were analyzed (75.47% PD, 24.53% DP) at median follow-up 17.88 months. Average age was 62.62 years, 51.78% were male, and surgery was for malignancy in 74.35% of patients. Post-operative endocrine insufficiency was present in 20.15% (n = 346). Male gender (p = 0.015), increased body mass index (BMI) (p < 0.001), tobacco use (p = 0.011), family history of diabetes (DM) (p < 0.001), personal history of DM (p ≤ 0.001), and DP (p ≤ 0.001) were correlated with increased risk. Mean time to onset was 20.80 ± 33.60 (IQR: 0.49-28.37) months. Post-operative exocrine insufficiency was present in 36.23% (n = 622). Race (p = 0.014), lower BMI (p < 0.001), family history of DM (p = 0.007), steatorrhea (p < 0.001), elevated pre-operative bilirubin (p = 0.019), and PD (p ≤ 0.001) were correlated with increased risk. Mean time to onset was 14.20 ± 26.90 (IQR: 0.89-12.69) months.
Conclusions: In this large series of pancreatectomy patients, 20.15% and 36.23% of patients developed post-operative endocrine and exocrine insufficiency at a mean time to onset of 20.80 and 14.20 months, respectively. Patients should be educated regarding post-resection insufficiencies and providers should have heightened awareness long-term.
Keywords: Distal pancreatectomy; Pancreatic endocrine insufficiency; Pancreatic enzyme replacement; Pancreatic exocrine insufficiency; Pancreaticoduodenectomy.
Figures
References
-
- Cameron JL. He J Two thousand consecutive pancreaticoduodenectomies. J Am Coll Surg. 2015;220:530–536. - PubMed
-
- Venkat R, Edil BH, Schulick RD, Lidor AO, Makary MA, Wolfgang CL. Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: A systematic review and meta-analysis. Ann Surg. 2012;255:1048–1059. - PubMed
-
- Cherif R, Gaujoux S, Couvelard A, Dokmak S, Vuillerme MP, Ruszniewski P, Belghiti J, Sauvanet A. Parenchyma-sparing resections for pancreatic neuroendocrine tumors. J Gastrointest Surg. 2012;16:2045–2055. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
