

Lymphocyte to Monocyte Ratio Predicts Resectability and Early Recurrence of Bismuth-Corlette Type IV Hilar Cholangiocarcinoma
- PMID: 30671792
- PMCID: PMC7026310
- DOI: 10.1007/s11605-018-04086-9
Lymphocyte to Monocyte Ratio Predicts Resectability and Early Recurrence of Bismuth-Corlette Type IV Hilar Cholangiocarcinoma
Abstract
Background: The objective of our research was to investigate the value of the lymphocyte to monocyte ratio (LMR) and its dynamic changes (LMRc) in predicting tumor resectability and early recurrence of radiologically resectable type IV hilar cholangiocarcinoma (HC).
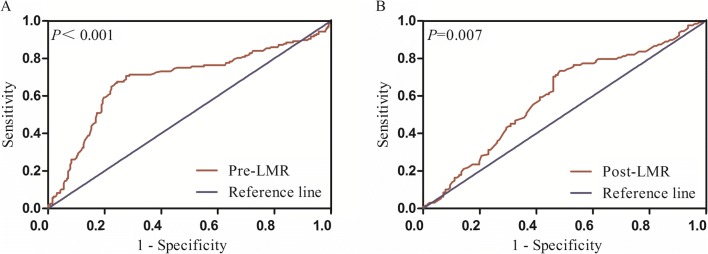
Methods: A total of 411 patients with radiologically resectable type IV HC were included. Data on their clinicopathologic characteristics, perioperative features, and survival outcomes were analyzed. Receiver operating characteristic (ROC) analysis was conducted to assess the ability of preoperative LMR (pre-LMR) to predict tumor resectability, and the ability of postoperative LMR (post-LMR) to discriminate between early and late recurrence. Survival curves were calculated using the Kaplan-Meier estimate. Univariate and multivariate logistic regression models were used to identify factors associated with resectability and early recurrence.
Results: Of 411 patients with potentially curative type IV HC, 254 underwent curative surgery. The optimal cutoff value of pre-LMR as an indicator of resectability was 3.67, and the optimal cutoff value of post-LMR for detecting early recurrence was 4.10. In the multivariate logistic regression model, CA19-9 > 200 U/mL, pre-LMR ≤ 3.67, and tumor size > 3 cm were found to be independent risk factors for poor resectability. Moreover, multivariate analysis showed that LMRc, resection margin, AJCC N stage, and lymphovascular invasion were independent risk factors associated with early recurrence.
Discussion: Pre-LMR is a valuable indicator of resectability and LMRc is a valuable predictor of early recurrence in patients with curative type IV HC.
Keywords: Bismuth-Corlette classification; Early recurrence; Hilar cholangiocarcinoma; Lymphocyte to monocyte ratio; Resectability.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
