

Assessment of the Relationship Between Genetic Determinants of Thyroid Function and Atrial Fibrillation: A Mendelian Randomization Study
- PMID: 30673084
- PMCID: PMC6396813
- DOI: 10.1001/jamacardio.2018.4635
Assessment of the Relationship Between Genetic Determinants of Thyroid Function and Atrial Fibrillation: A Mendelian Randomization Study
Abstract
Importance: Increased free thyroxine (FT4) and decreased thyrotropin are associated with increased risk of atrial fibrillation (AF) in observational studies, but direct involvement is unclear.
Objective: To evaluate the potential direct involvement of thyroid traits on AF.
Design, setting, and participants: Study-level mendelian randomization (MR) included 11 studies, and summary-level MR included 55 114 AF cases and 482 295 referents, all of European ancestry.
Exposures: Genomewide significant variants were used as instruments for standardized FT4 and thyrotropin levels within the reference range, standardized triiodothyronine (FT3):FT4 ratio, hypothyroidism, standardized thyroid peroxidase antibody levels, and hyperthyroidism. Mendelian randomization used genetic risk scores in study-level analysis or individual single-nucleotide polymorphisms in 2-sample MR for the summary-level data.
Main outcomes and measures: Prevalent and incident AF.
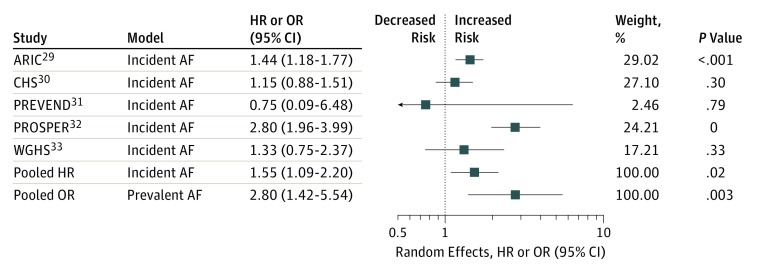
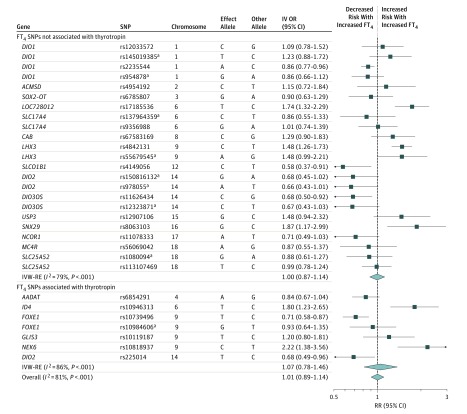
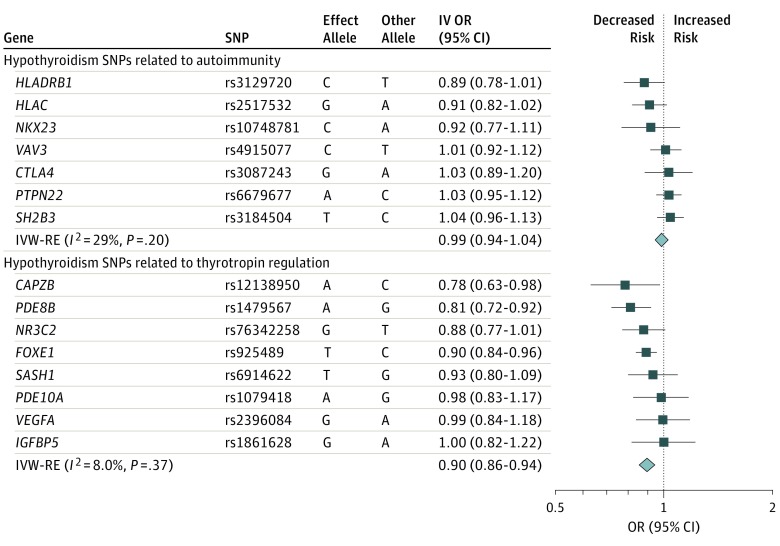
Results: The study-level analysis included 7679 individuals with AF and 49 233 referents (mean age [standard error], 62 [3] years; 15 859 men [29.7%]). In study-level random-effects meta-analysis, the pooled hazard ratio of FT4 levels (nanograms per deciliter) for incident AF was 1.55 (95% CI, 1.09-2.20; P = .02; I2 = 76%) and the pooled odds ratio (OR) for prevalent AF was 2.80 (95% CI, 1.41-5.54; P = .003; I2 = 64%) in multivariable-adjusted analyses. The FT4 genetic risk score was associated with an increase in FT4 by 0.082 SD (standard error, 0.007; P < .001) but not with incident AF (risk ratio, 0.84; 95% CI, 0.62-1.14; P = .27) or prevalent AF (OR, 1.32; 95% CI, 0.64-2.73; P = .46). Similarly, in summary-level inverse-variance weighted random-effects MR, gene-based FT4 within the reference range was not associated with AF (OR, 1.01; 95% CI, 0.89-1.14; P = .88). However, gene-based increased FT3:FT4 ratio, increased thyrotropin within the reference range, and hypothyroidism were associated with AF with inverse-variance weighted random-effects OR of 1.33 (95% CI, 1.08-1.63; P = .006), 0.88 (95% CI, 0.84-0.92; P < .001), and 0.94 (95% CI, 0.90-0.99; P = .009), respectively, and robust to tests of horizontal pleiotropy. However, the subset of hypothyroidism single-nucleotide polymorphisms involved in autoimmunity and thyroid peroxidase antibodies levels were not associated with AF. Gene-based hyperthyroidism was associated with AF with MR-Egger OR of 1.31 (95% CI, 1.05-1.63; P = .02) with evidence of horizontal pleiotropy (P = .045).
Conclusions and relevance: Genetically increased FT3:FT4 ratio and hyperthyroidism, but not FT4 within the reference range, were associated with increased AF, and increased thyrotropin within the reference range and hypothyroidism were associated with decreased AF, supporting a pathway involving the pituitary-thyroid-cardiac axis.
Conflict of interest statement
Figures

Comment in
-
Thyroid Function and the Risk of Atrial Fibrillation: Exploring Potentially Causal Relationships Through Mendelian Randomization.JAMA Cardiol. 2019 Feb 1;4(2):97-99. doi: 10.1001/jamacardio.2018.4614. JAMA Cardiol. 2019. PMID: 30673080 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
