

Imaging Patterns Are Associated with Interstitial Lung Abnormality Progression and Mortality
- PMID: 30673508
- PMCID: PMC6635786
- DOI: 10.1164/rccm.201809-1652OC
Imaging Patterns Are Associated with Interstitial Lung Abnormality Progression and Mortality
Abstract
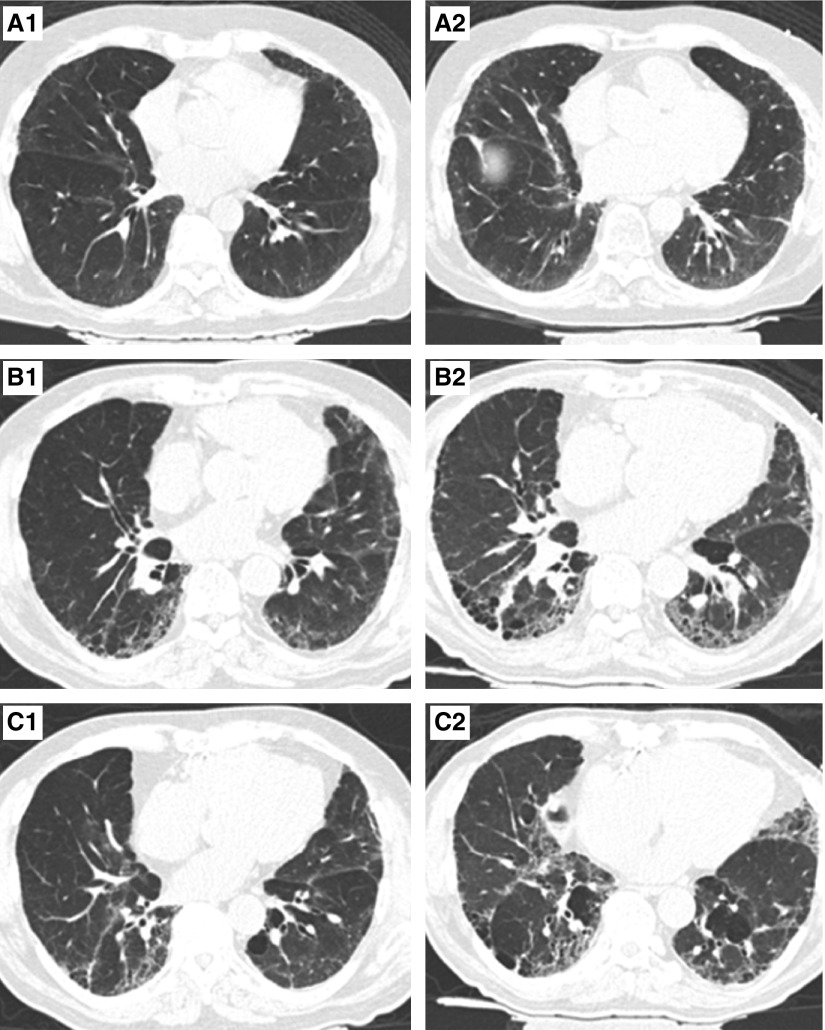
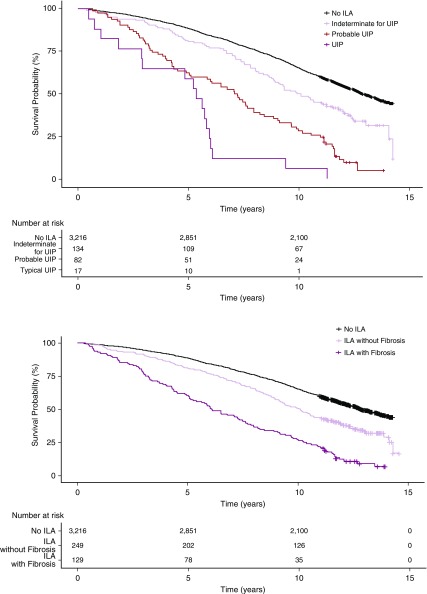
Rationale: Interstitial lung abnormalities (ILA) are radiologic abnormalities on chest computed tomography scans that have been associated with an early or mild form of pulmonary fibrosis. Although ILA have been associated with radiologic progression, it is not known if specific imaging patterns are associated with progression or risk of mortality. Objectives: To determine the role of imaging patterns on the risk of death and ILA progression. Methods: ILA (and imaging pattern) were assessed in 5,320 participants from the AGES-Reykjavik Study, and ILA progression was assessed in 3,167 participants. Multivariable logistic regression was used to assess factors associated with ILA progression, and Cox proportional hazards models were used to assess time to mortality. Measurements and Main Results: Over 5 years, 327 (10%) had ILA on at least one computed tomography, and 1,435 (45%) did not have ILA on either computed tomography. Of those with ILA, 238 (73%) had imaging progression, whereas 89 (27%) had stable to improved imaging; increasing age and copies of MUC5B genotype were associated with imaging progression. The definite fibrosis pattern was associated with the highest risk of progression (odds ratio, 8.4; 95% confidence interval, 2.7-25; P = 0.0003). Specific imaging patterns were also associated with an increased risk of death. After adjustment, both a probable usual interstitial pneumonia and usual interstitial pneumonia pattern were associated with an increased risk of death when compared with those indeterminate for usual interstitial pneumonia (hazard ratio, 1.7; 95% confidence interval, 1.2-2.4; P = 0.001; hazard ratio, 3.9; 95% confidence interval, 2.3-6.8;P < 0.0001), respectively. Conclusions: In those with ILA, imaging patterns can be used to help predict who is at the greatest risk of progression and early death.
Keywords: idiopathic pulmonary fibrosis; imaging pattern; interstitial lung abnormalities; mortality; progression.
Figures
Comment in
-
Subclinical Interstitial Lung Abnormalities: Lumping and Splitting Revisited.Am J Respir Crit Care Med. 2019 Jul 15;200(2):121-123. doi: 10.1164/rccm.201901-0180ED. Am J Respir Crit Care Med. 2019. PMID: 30699307 Free PMC article. No abstract available.
References
-
- Putman RK, Hatabu H, Araki T, Gudmundsson G, Gao W, Nishino M, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators; COPDGene Investigators. Association between interstitial lung abnormalities and all-cause mortality. JAMA. 2016;315:672–681. - PMC - PubMed
-
- Miller ER, Putman RK, Vivero M, Hung Y, Araki T, Nishino M, et al. Interstitial lung abnormalities and histopathologic correlates in patients undergoing lung nodule resection [abstract] Am J Respir Crit Care Med. 2017;195:A1120.
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL113264/HL/NHLBI NIH HHS/United States
- R01 HL130974/HL/NHLBI NIH HHS/United States
- U01 HL133232/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- R01 HL135142/HL/NHLBI NIH HHS/United States
- R01 HL137927/HL/NHLBI NIH HHS/United States
- T32 HL007085/HL/NHLBI NIH HHS/United States
- R01 HL097163/HL/NHLBI NIH HHS/United States
- R33 HL120770/HL/NHLBI NIH HHS/United States
- R01 CA203636/CA/NCI NIH HHS/United States
- P01 HL114501/HL/NHLBI NIH HHS/United States
- R01 HL122464/HL/NHLBI NIH HHS/United States
- P01 HL092870/HL/NHLBI NIH HHS/United States
- K08 HL140087/HL/NHLBI NIH HHS/United States
- R01 HL111024/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
