

European Practical and Patient-Centred Guidelines for Adult Obesity Management in Primary Care
- PMID: 30673677
- PMCID: PMC6465693
- DOI: 10.1159/000496183
European Practical and Patient-Centred Guidelines for Adult Obesity Management in Primary Care
Abstract
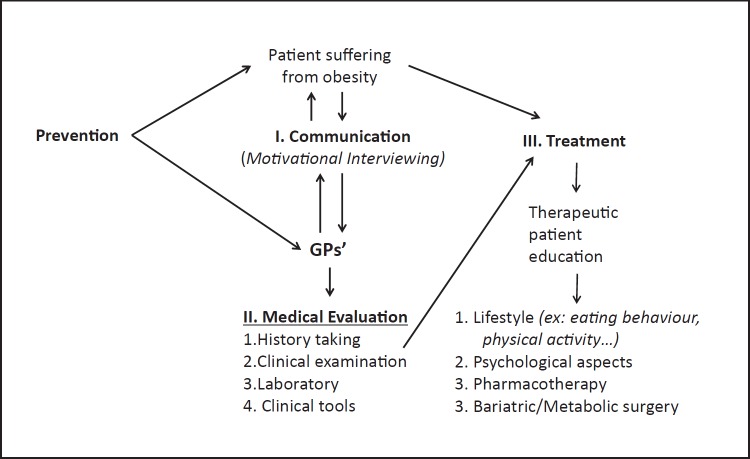
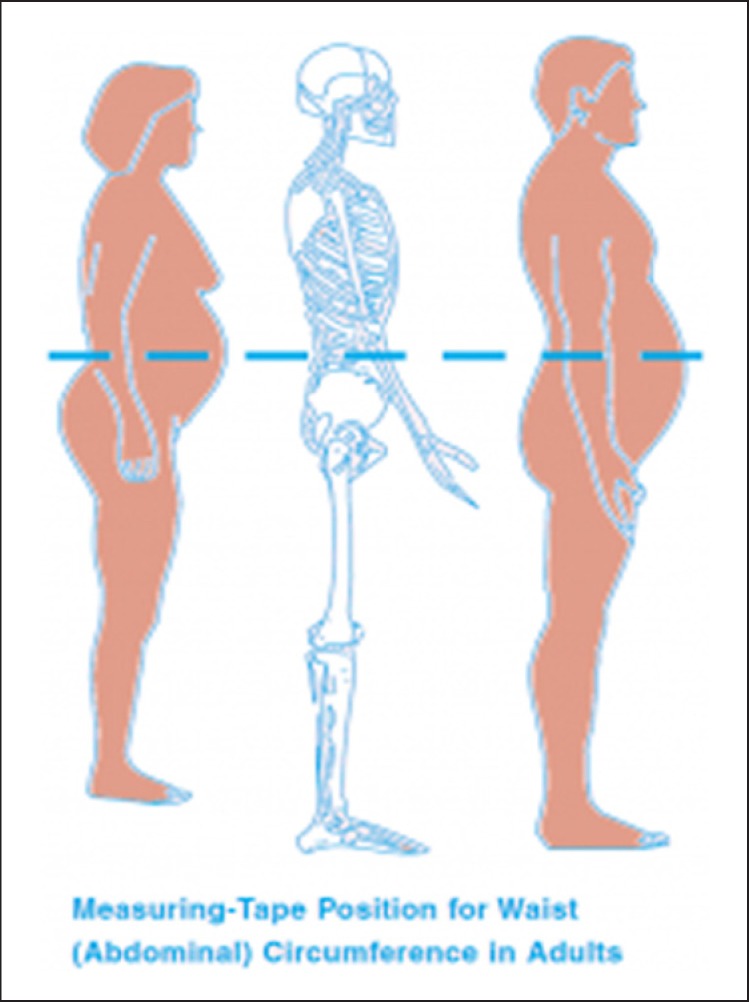
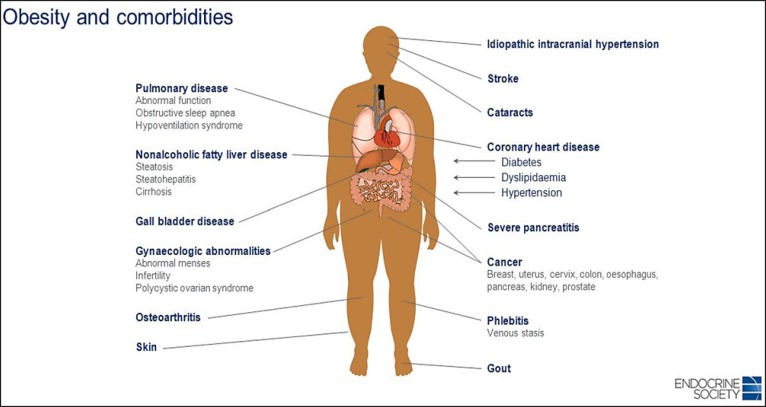
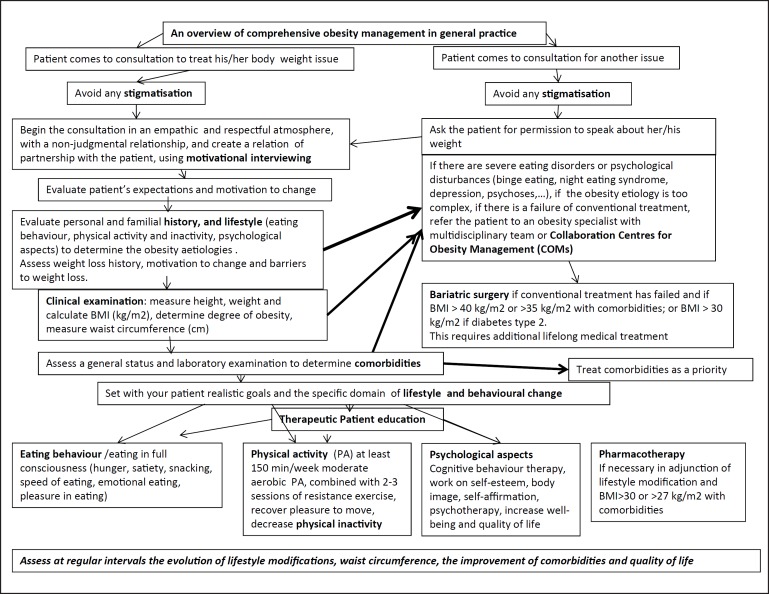
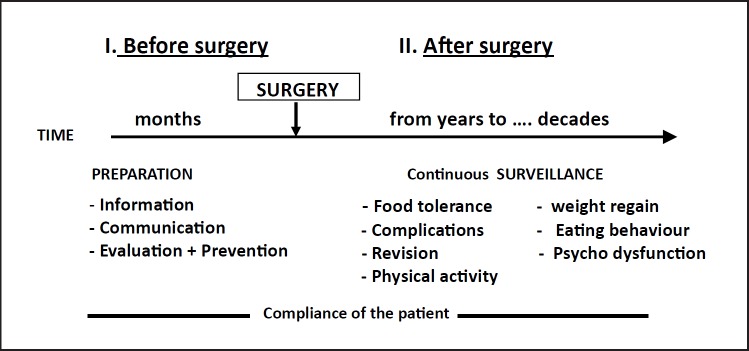
The first contact for patients with obesity for any medical treatment or other issues is generally with General Practitioners (GPs). Therefore, given the complexity of the disease, continuing GPs' education on obesity management is essential. This article aims to provide obesity management guidelines specifically tailored to GPs, favouring a practical patient-centred approach. The focus is on GP communication and motivational interviewing as well as on therapeutic patient education. The new guidelines highlight the importance of avoiding stigmatization, something frequently seen in different health care settings. In addition, managing the psychological aspects of the disease, such as improving self-esteem, body image and quality of life must not be neglected. Finally, the report considers that achieving maximum weight loss in the shortest possible time is not the key to successful treatment. It suggests that 5-10% weight loss is sufficient to obtain substantial health benefits from decreasing comorbidities. Reducing waist circumference should be considered even more important than weight loss per se, as it is linked to a decrease in visceral fat and associated cardiometabolic risks. Finally, preventing weight regain is the cornerstone of lifelong treatment, for any weight loss techniques used (behavioural or pharmaceutical treatments or bariatric surgery).
Keywords: Bariatric/metabolic surgery; Behavioural therapy; Conservative treatment; GPs; Management; Motivational interviewing; Obesity; Overweight; Primary care.
© 2019 The Author(s) Published by S. Karger AG, Basel.
Figures

References
-
- Collaboration NC, NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in body-mass indexunderweight, overweight and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children adolescents, and adults. Lancet. 2017 Dec;390((10113)):2627–42. - PMC - PubMed
-
- Timothy Garvey W. 2016. MD, and Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines AACE/ACE Guidelines American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity, - PubMed
-
- National Institutes of Health The Practical Guide: Identification Evaluation, and Treatment of Overweight and Obesity in Adults. NHLBI Obesity Education Initiative Expert Panel on the Identification Evaluation, and Treatment of Overweight and Obesity in Adults. Bethesda, NIH, 2000 www.nhlbi.nih.gov/files/docs/guidelines/prctgd_c.pdf (accessed November 30, 2015)
-
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines Obesity Society: 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014; 129 (suppl 2): S102–S138. Erratum in Circulation. 2014;129(suppl 2):S139–40. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
