

Superior mesenteric artery syndrome coexists with Nutcracker syndrome in a female: a case report
- PMID: 30674275
- PMCID: PMC6343343
- DOI: 10.1186/s12876-019-0932-1
Superior mesenteric artery syndrome coexists with Nutcracker syndrome in a female: a case report
Abstract
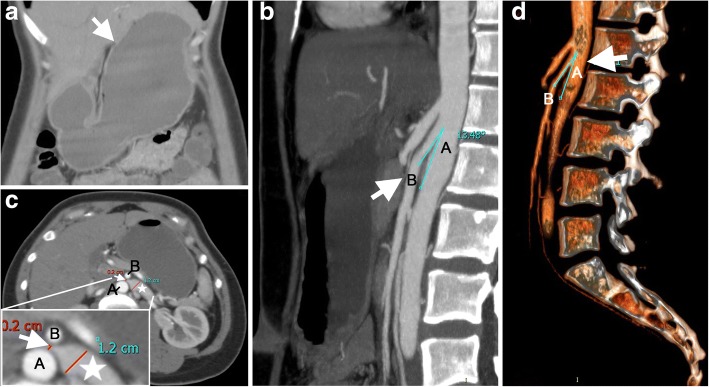
Background: Superior mesenteric artery (SMA) syndrome, also known as Wilkie's syndrome or Benign duodenal stasis, is a rare benign disease. It could threaten the life if the manifestation is severe and the treatment is inappropriate. In the patients with SMA syndrome, the third portion (transverse part) of the duodenum is compressed externally between the SMA and abdominal aorta (AA) leading to duodenal stasis and gastrointestinal obstruction. SMA syndrome may rarely combine with Nutcracker syndrome when left renal vein (LRV) was compressed between SMA and AA.
Case presentation: A 32-year-old female patient presented with complaints of gradually severe bloating, epigastric pain, left flank ache, nausea and occasional vomiting of 1 month's duration. The epigastric and left flank ache was aggravated when the patient was supine and relieved in a prone or left lateral decubitus. The abdominal bloating was associated with early satiety. The vomiting always started 40 min after meal. The patient gave a history of urine stone with drotaverine hydrochloride tablets treatment for two weeks before the gastrointestinal symptoms arising. The patient had no significant surgical history, but had a rapid weight loss of approximately 10 kg with a body mass index (BMI) from 21 kg/m2 to less than 18 kg/m2 over the last two months. An abdominal examination revealed upper abdominal tenderness and distention. The urine routine examination showed no significant abnormality. The findings of initial blood tests and other laboratory investigations were unremarkable.
Conclusions: This case reports a female patient with SMA syndrome with Nutcracker syndrome predisposed by Antispasmodics. We highlight the importance of the combination therapy of long-term nutritional supporting and prokinetic agents. Rehabilitating practice after discharge is beneficial to reduce recurrence.
Keywords: Nutcracker syndrome; Superior mesenteric artery.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Ganss A, Rampado S, Savarino E, Bardini R. Superior mesenteric artery syndrome: a prospective study in a single institution. J Gastrointest Surg. 2018. 10.1007/s11605-018-3984-6. Accessed 5 Oct 2018. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
