

The association between endometrial thickness and pregnancy outcome in gonadotropin-stimulated intrauterine insemination cycles
- PMID: 30674305
- PMCID: PMC6345006
- DOI: 10.1186/s12958-019-0455-1
The association between endometrial thickness and pregnancy outcome in gonadotropin-stimulated intrauterine insemination cycles
Abstract
Background: Intrauterine insemination (IUI) is the first-line treatment for non-tubal infertility. Injectable gonadotropins are often chosen as adjunctive stimulation to promote the growth of ovarian follicles in IUI cycles. The growing follicles produce estrogen, which induces endometrial proliferation and increased endometrial stripe thickness (EST). The association between EST and pregnancy outcome in gonadotropin stimulated IUI is not well studied. The objective of this study is to determine if EST can predict pregnancy outcome in gonadotropin-stimulated IUI cycles.
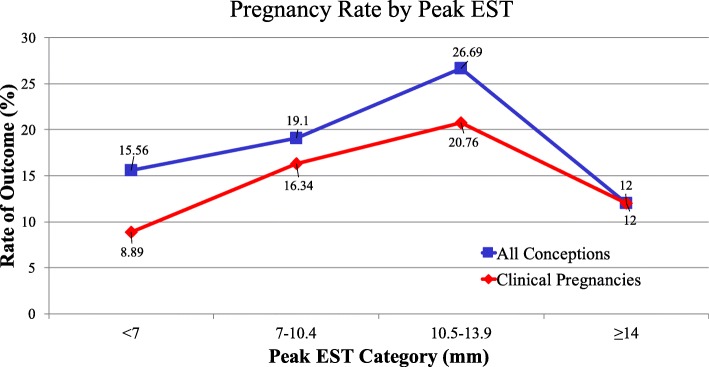
Methods: A retrospective review was conducted of all exclusively gonadotropin-stimulated IUI cycles performed between 2012 and 2015 at an academic fertility clinic. Mean endometrial thickness was compared in positive versus negative cycles using Student T-test. Peak EST values were then divided into four groups of < 7 mm, 7.0-10.4 mm, 10.5-13.9 mm, and ≥ 14 mm. Multiple logistic regression analysis adjusted for potential confounders was conducted to assess the impact of peak EST on cycle outcome.
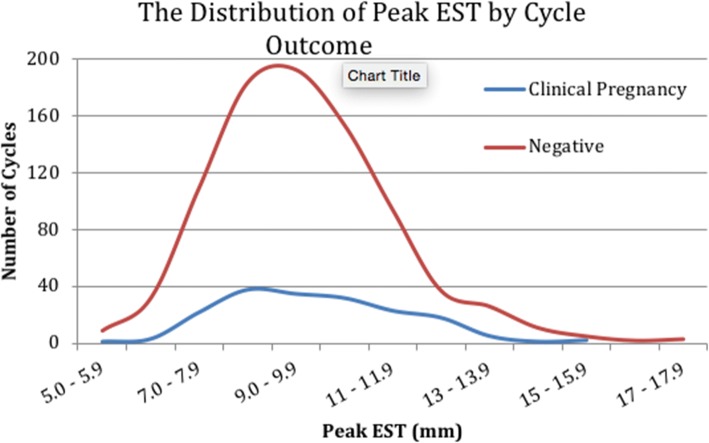
Results: Our sample consisted of 1065 IUI cycles representing 548 patients with a 16.9% clinical pregnancy rate and 20.5% conception rate. No significant differences in mean peak EST were observed between cycles that achieved clinical pregnancy or conception and those that did not. Division of peak EST into four groups showed a non-linear relationship between peak EST and cycle outcome, with highest rates of positive outcomes between 10.5-13.9 mm. The odds of clinical pregnancy and conception increased by 38 and 44% respectively with each subsequent peak EST category up to 10.5-13.9 mm, following which they declined.
Conclusion: This is the largest study to date evaluating the effect of peak EST on gonadotropin-stimulated IUI cycles exclusively. The lack of significant difference in peak EST between positive and negative outcomes cycles may be due to the non-linear relationship between cycle outcomes and peak EST. Peak EST in the range of 10.5-13.9 mm was associated with significantly higher conception rates and a trend towards higher clinical pregnancy rates. This non-linearity is likely one of the reasons that EST in isolation was found to be a poor predictor of IUI outcomes, and therefore is not appropriate to be used as the sole indicator for cycle cancellation.
Keywords: Clinical pregnancy; Endometrial stripe thickness; Injectable gonadotropins; Intrauterine insemination; Pregnancy outcome.
Conflict of interest statement
Author information
CC is a Clinician Investigator at Mount Sinai Hospital and an Assistant Professor of Obstetrics and Gynecology at the University of Toronto. She is a Fellow of the Royal College of Surgeons and Physicians of Canada, with dual specialization in Obstetrics and Gynecology and REI.
Ethics approval and consent
Ethical approval was granted through the Mount Sinai Hospital Research Ethics Board. Consent to participate is not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
