

Safety and prognostic value of regadenoson stress cardiovascular magnetic resonance imaging in heart transplant recipients
- PMID: 30674318
- PMCID: PMC6345066
- DOI: 10.1186/s12968-018-0515-2
Safety and prognostic value of regadenoson stress cardiovascular magnetic resonance imaging in heart transplant recipients
Abstract
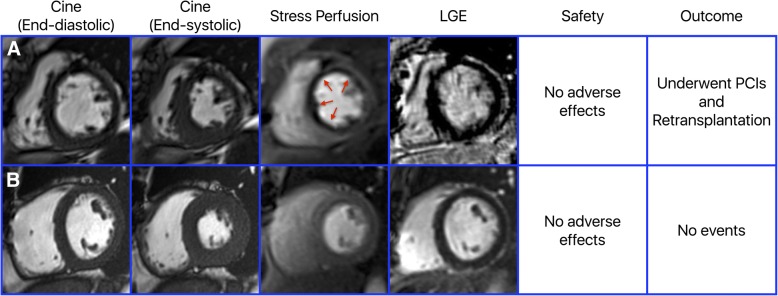
Background: There is a critical need for non-invasive methods to detect coronary allograft vasculopathy and to risk stratify heart transplant recipients. Vasodilator stress testing using cardiovascular magnetic resonance imaging (CMR) is a promising technique for this purpose. We aimed to evaluate the safety and the prognostic value of regadenoson stress CMR in heart transplant recipients.
Methods: To evaluate the safety, we assessed adverse effects in a retrospective matched cohort study of consecutive heart transplant recipients who underwent regadenoson stress CMR matched in a 2:1 ratio to age- and gender-matched non-heart transplant patients. To evaluate the prognostic value, we compared the outcomes of patients with abnormal vs. normal regadenoson stress CMRs using a composite endpoint of myocardial infarction, percutaneous intervention, cardiac hospitalization, retransplantation or death.
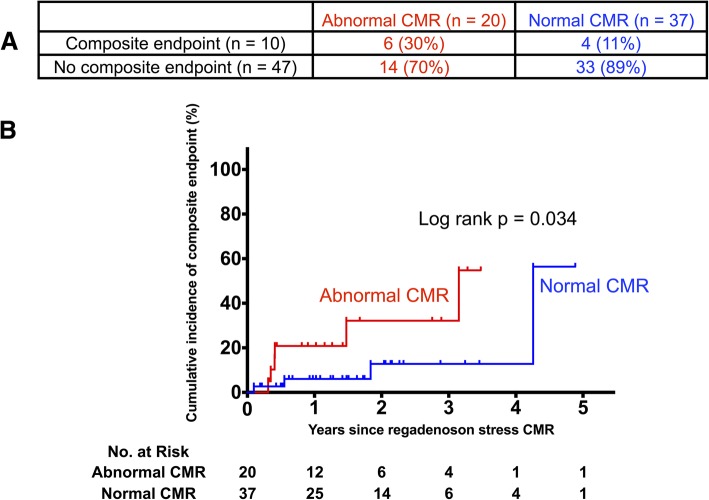
Results: For the safety analysis, 234 regadenoson stress CMR studies were included - 78 performed in 57 heart transplant recipients and 156 performed in non-heart transplant patients. Those in heart transplant recipients were performed at a median of 2.74 years after transplantation. Thirty-four (44%) CMR studies were performed in the first two years after heart transplantation. There were no differences in the rates of adverse effects between heart transplant recipients and non-heart transplant patients. To study the prognostic value of regadenoson stress CMRs, 20 heart transplant recipients with abnormal regadenoson stress CMRs were compared to 37 with normal regadenoson stress CMRs. An abnormal regadenoson stress CMR was associated with a significantly higher incidence of the composite endpoint compared with a normal regadenoson stress CMR (3-year cumulative incidence estimates of 32.1% vs. 12.7%, p = 0.034).
Conclusions: Regadenoson stress CMR is safe and well tolerated in heart transplant recipients, with no incidence of sinus node dysfunction or high-degree atrioventricular block, including in the first two years after heart transplantation. An abnormal regadenoson stress CMR identifies heart transplant recipients at a higher risk for major adverse cardiovascular events.
Keywords: Cardiovascular magnetic resonance; Regadenoson; Safety; Stress perfusion; Vasodilator.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by University of Minnesota’s Institutional Review Board with a waiver of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Lund LH, Edwards LB, Dipchand AI, Goldfarb S, Kucheryavaya AY, Levvey BJ, Meiser B, Rossano JW, Yusen RD, Stehlik J, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-third adult heart transplantation Report-2016; focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant. 2016;35:1158–1169. doi: 10.1016/j.healun.2016.08.017. - DOI - PubMed
-
- Estep JD, Shah DJ, Nagueh SF, Mahmarian JJ, Torre-Amione G, Zoghbi WA. The role of multimodality cardiac imaging in the transplanted heart. JACC Cardiovasc Imaging. 2009;2:1126–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
