

Impact and sustainability of centralising acute stroke services in English metropolitan areas: retrospective analysis of hospital episode statistics and stroke national audit data
- PMID: 30674465
- PMCID: PMC6334718
- DOI: 10.1136/bmj.l1
Impact and sustainability of centralising acute stroke services in English metropolitan areas: retrospective analysis of hospital episode statistics and stroke national audit data
Abstract
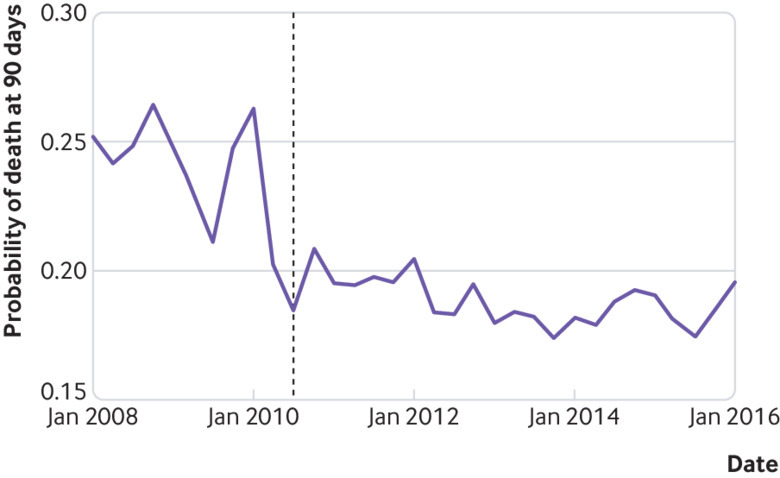
Objectives: To investigate whether further centralisation of acute stroke services in Greater Manchester in 2015 was associated with changes in outcomes and whether the effects of centralisation of acute stroke services in London in 2010 were sustained.
Design: Retrospective analyses of patient level data from the Hospital Episode Statistics (HES) database linked to mortality data from the Office for National Statistics, and the Sentinel Stroke National Audit Programme (SSNAP).
Setting: Acute stroke services in Greater Manchester and London, England.
Participants: 509 182 stroke patients in HES living in urban areas admitted between January 2008 and March 2016; 218 120 stroke patients in SSNAP between April 2013 and March 2016.
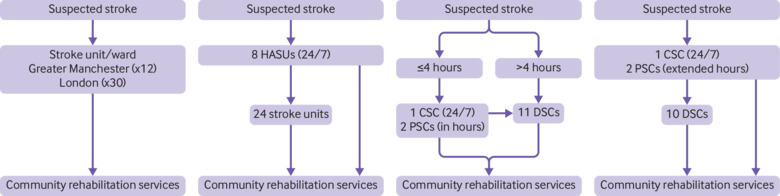
Interventions: Hub and spoke models for acute stroke care.
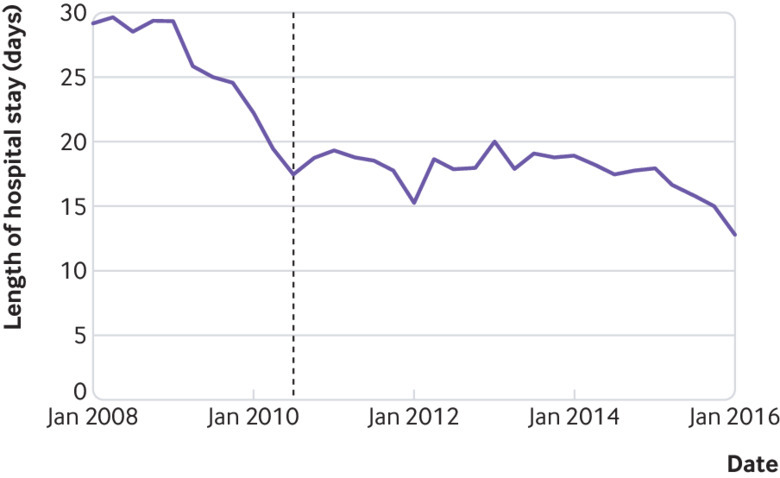
Main outcome measures: Mortality at 90 days after hospital admission; length of acute hospital stay; treatment in a hyperacute stroke unit; 19 evidence based clinical interventions.
Results: In Greater Manchester, borderline evidence suggested that risk adjusted mortality at 90 days declined overall; a significant decline in mortality was seen among patients treated at a hyperacute stroke unit (difference-in-differences -1.8% (95% confidence interval -3.4 to -0.2)), indicating 69 fewer deaths per year. A significant decline was seen in risk adjusted length of acute hospital stay overall (-1.5 (-2.5 to -0.4) days; P<0.01), indicating 6750 fewer bed days a year. The number of patients treated in a hyperacute stroke unit increased from 39% in 2010-12 to 86% in 2015/16. In London, the 90 day mortality rate was sustained (P>0.05), length of hospital stay declined (P<0.01), and more than 90% of patients were treated in a hyperacute stroke unit. Achievement of evidence based clinical interventions generally remained constant or improved in both areas.
Conclusions: Centralised models of acute stroke care, in which all stroke patients receive hyperacute care, can reduce mortality and length of acute hospital stay and improve provision of evidence based clinical interventions. Effects can be sustained over time.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work other than that described above; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; AGR is national clinical director for stroke in England and clinical director for stroke in London; PJT was clinical lead for stroke in Greater Manchester up to 2013 and led the Greater Manchester stroke service redesign from 2007 until 2012.
Figures
References
-
- Feigin VL, Roth GA, Naghavi M, et al. Global Burden of Diseases, Injuries and Risk Factors Study 2013 and Stroke Experts Writing Group Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol 2016;15:913-24. 10.1016/S1474-4422(16)30073-4 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous