

How I treat refractory chronic graft-versus-host disease
- PMID: 30674472
- PMCID: PMC6418480
- DOI: 10.1182/blood-2018-04-785899
How I treat refractory chronic graft-versus-host disease
Abstract
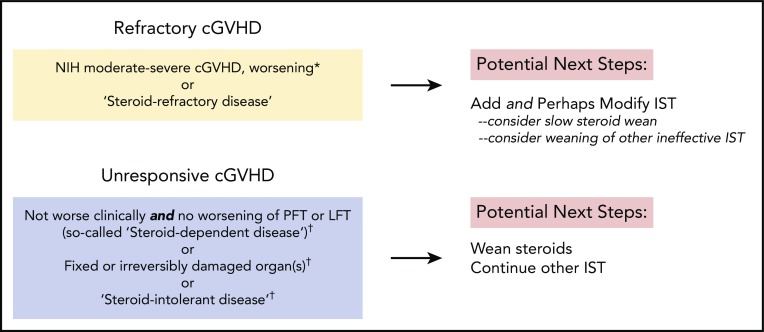
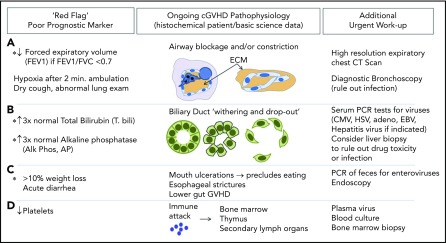
Approximately 35% to 50% of patients otherwise cured of hematologic malignancies after allogeneic hematopoietic stem cell transplantation will develop the pleomorphic autoimmune-like syndrome known as chronic graft-versus-host disease (cGVHD). Since in 2005, National Institutes of Health (NIH) consensus panels have proposed definitions and classifications of disease to standardize treatment trials. Recently, the first agent was approved by the US Food and Drug Administration for steroid-refractory cGVHD. Despite these advances, most individuals do not achieve durable resolution of disease activity with initial treatment. Moreover, standardized recommendations on how to best implement existing and novel immunomodulatory agents and taper salvage agents are often lacking. Given the potential life-threatening nature of cGVHD, we employ in our practice patient assessment templates at each clinic visit to elucidate known prognostic indicators and red flags. We find NIH scoring templates practical for ongoing assessments of these complex patient cases and determination of when changes in immunosuppressive therapy are warranted. Patients not eligible or suitable for clinical trials have systemic and organ-directed adjunctive treatments crafted in a multidisciplinary clinic. Herein, we review these treatment options and offer a management and monitoring scaffold for representative patients with cGVHD not responding to initial therapy.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.S. received a research grant from Gilead and served on advisory boards for Pharmacyclics. The remaining authors declare no competing financial interests.
Figures
References
-
- Graze PR, Gale RP. Chronic graft versus host disease: a syndrome of disordered immunity. Am J Med. 1979;66(4):611-620. - PubMed
-
- Shulman HM, Sullivan KM, Weiden PL, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69(2):204-217. - PubMed
-
- Sullivan KM, Shulman HM, Storb R, et al. Chronic graft-versus-host disease in 52 patients: adverse natural course and successful treatment with combination immunosuppression. Blood. 1981;57(2):267-276. - PubMed
-
- Soiffer RJ, Kim HT, McGuirk J, et al. Prospective, randomized, double-blind, phase III clinical trial of anti-T-lymphocyte globulin to assess impact on chronic graft-versus-host disease-free survival in patients undergoing HLA-matched unrelated myeloablative hematopoietic cell transplantation. J Clin Oncol. 2017;35(36):4003-4011. - PMC - PubMed
-
- Kröger N, Solano C, Wolschke C, et al. Antilymphocyte globulin for prevention of chronic graft-versus-host disease. N Engl J Med. 2016;374(1):43-53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
