

Claims data analyses unable to properly characterize the value of neurologists in epilepsy care
- PMID: 30674587
- PMCID: PMC6404473
- DOI: 10.1212/WNL.0000000000007004
Claims data analyses unable to properly characterize the value of neurologists in epilepsy care
Abstract
Objective: To determine the association of a neurologist visit with health care use and cost outcomes for patients with incident epilepsy.
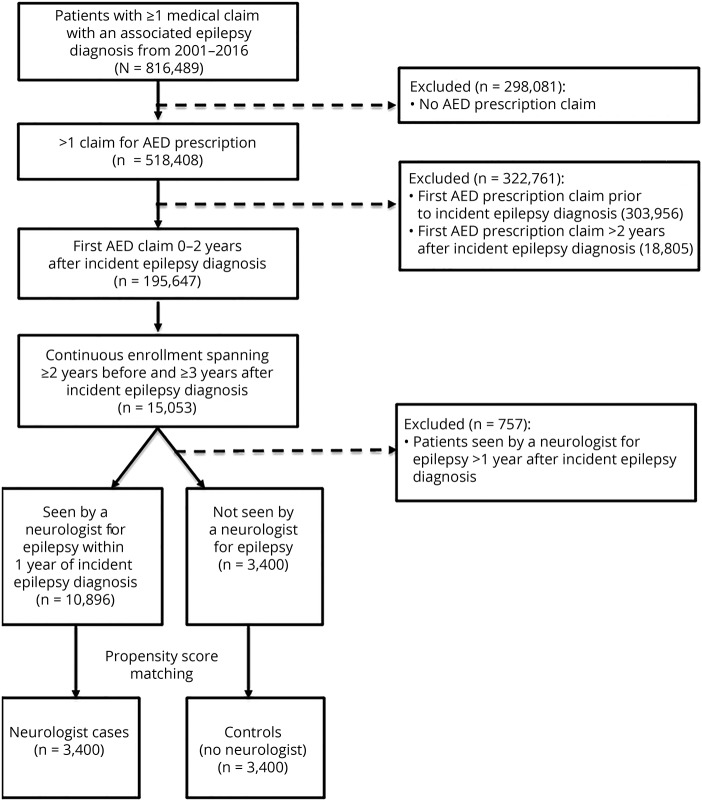
Methods: Using health care claims data for individuals insured by United Healthcare from 2001 to 2016, we identified patients with incident epilepsy. The population was defined by an epilepsy/convulsion diagnosis code (ICD codes 345.xx/780.3x, G40.xx/R56.xx), an antiepileptic prescription filled within the succeeding 2 years, and neither criterion met in the 2 preceding years. Cases were defined as patients who had a neurologist encounter for epilepsy within 1 year after an incident diagnosis; a control cohort was constructed with propensity score matching. Primary outcomes were emergency room (ER) visits and hospitalizations for epilepsy. Secondary outcomes included measures of cost (epilepsy related, not epilepsy related, and antiepileptic drugs) and care escalation (including EEG evaluation and epilepsy surgery).
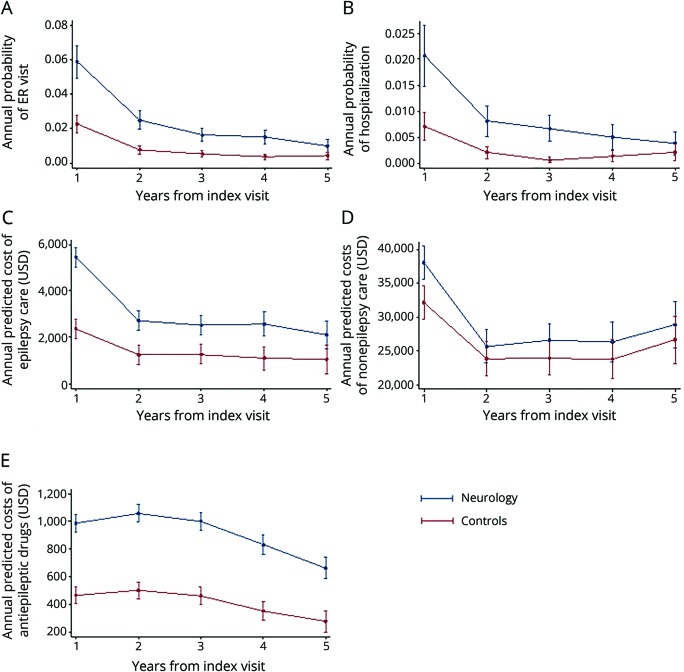
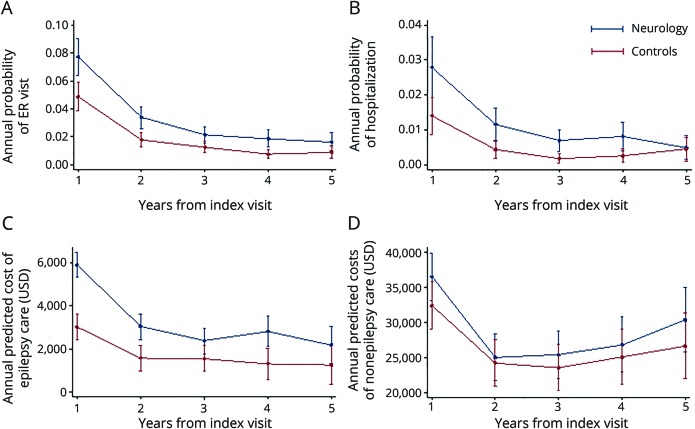
Results: After participant identification and propensity score matching, there were 3,400 cases and 3,400 controls. Epilepsy-related ER visits were more likely for cases than controls (year 1: 5.9% vs 2.3%, p < 0.001), as were hospitalizations (year 1: 2.1% vs 0.7%, p < 0.001). Total medical costs for epilepsy care, nonepilepsy care, and antiepileptic drugs were greater for cases (p ≤ 0.001). EEG evaluation and epilepsy surgery occurred more commonly for cases (p ≤ 0.001).
Conclusions: Patients with epilepsy who visited a neurologist had greater subsequent health care use, medical costs, and care escalation than controls. This comparison using administrative claims is plausibly confounded by case disease severity, as suggested by higher nonepilepsy care costs. Linking patient-centered outcomes to claims data may provide the clinical resolution to assess care value within a heterogeneous population.
© 2019 American Academy of Neurology.
Figures
References
-
- Gorelick PB. Adaptation of neurological practice and policy to a changing US health-care landscape. Lancet Neurol 2016;15:444–450. - PubMed
-
- England MJ, Liverman CT, Schultz AM, Strawbridge LM; Institute of Medicine Committee on Public Health Dimensions of the Epilepsies. Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: National Academies Press; 2012. - PubMed
-
- Gooch CL, Pracht E, Borenstein AR. The burden of neurological disease in the United States: a summary report and call to action. Ann Neurol 2017;81:479–484. - PubMed
-
- Begley CE, Durgin TL. The direct cost of epilepsy in the United States: a systematic review of estimates. Epilepsia 2015;56:1376–1387. - PubMed
-
- Begley CE, Famulari M, Annegers JF, et al. The cost of epilepsy in the United States: an estimate from population-based clinical and survey data. Epilepsia 2000;41:342–351. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous