

doi: 10.11909/j.issn.1671-5411.2018.12.005.
Characterization of coronary atherosclerotic plaques in a homozygous familial hypercholesterolemia visualized by optical coherence tomography
Affiliations
- PMID: 30675146
- PMCID: PMC6330271
- DOI: 10.11909/j.issn.1671-5411.2018.12.005
Item in Clipboard
Characterization of coronary atherosclerotic plaques in a homozygous familial hypercholesterolemia visualized by optical coherence tomography
J Geriatr Cardiol.
2018 Dec.
No abstract available
Keywords: Coronary atherosclerotic plaques; Homozygous familial hypercholesterolemia; Optical coherence tomography.
Figures


(A): The sequence of 1470 G >A nonsense mutation in exon 10 resulting in W469X; (B): the proband was indicated with an arrow. Squares indicate men; circles, women; deceased persons were indicated by a diagonal line drawn through the symbol. LDL-C: low-density lipoprotein cholesterol.

HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TC: total cholesterol; TG: triglyceride.

(A): Left ventricle ejection fraction was 68.9% with no wall motion abnormalities; (B): severe aortic valve calcification was found in non-coronary cusp (white arrow head); (C): severe aortic valve calcification was found in Left coronary cusp (white arrow head).

(A): Multiple calcified plaques were noted in the aortic root and a non-calcified plaque was noted in the origin of RCA (white arrow head); (B): multiple mixed plaques and calcified plaque were noted all across RCA. The calcified plaque located in the middle of the RCA resulted in severe stenosis (white arrow head); (C): the main segment of the left coronary is normal. Multiple calcified plaques and non-calcified plaques were noted in the proximal segment of LAD, which resulted in severe stenosis (white arrowhead); (D): multiple non-calcified plaques were noted in the proximal. CTCA: computed tomography coronary angiography; LAD: left anterior descending; LCX: left circumflex artery; RCA: right coronary artery.
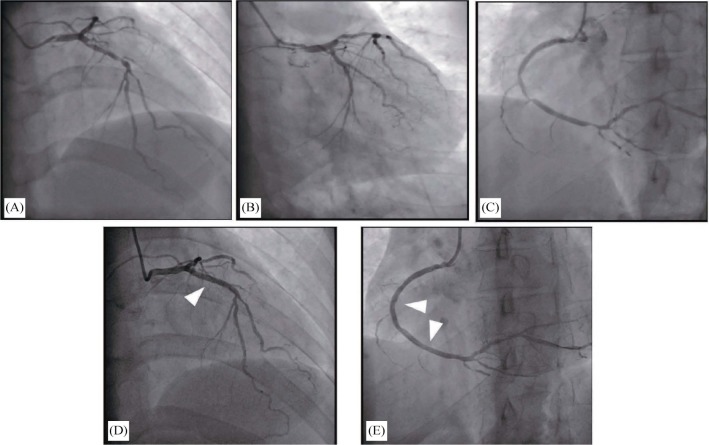
(A): Diffuse stenosis in proximal and middle LAD, with the uttermost of 90% stenosis; (B): the distal of LCX was total occlusion; (C): diffuse stenosis all across RCA, with 90% stenosis in middle and distal RCA; (D): a stent was implanted in the culprit lesion of LAD (arrow head); (E): two stents were implanted in the RCA (arrow head). LAD: left anterior descending; RCA: right coronary artery.

(A): An intact three-layer structure of the vessel wall; (B): a thin-cap fibroatheroma was located in the middle segment of RCA. The least fibrous cap thickness was 40 µm and the lipid core occupied two quadrants; (C): fibrous hyperplasia mixed with calcification in the narrowest part of RCA; (D): severe fibrous hyperplasia; (E): an intact three-layer structure of the vessel wall; (F): lipid plaque accompanied with inflammatory cell infiltration; (G): a large lipid plaque in the narrowest site of LAD; (H): mixed plaque accompanied with inflammatory cell infiltration; (I): calcified plaque; (J): normal vessel. LAD: left anterior descending; OCT: optical coherence tomography; RCA: right coronary artery.
Similar articles
-
Percutaneous coronary intervention for a Chinese familial hypercholesterolemia homozygous under the guidance of optical coherence tomography.Atheroscler Suppl. 2019 Mar;36:19-23. doi: 10.1016/j.atherosclerosissup.2019.01.004. Atheroscler Suppl. 2019. PMID: 30876528
-
Visualization of coronary atherosclerotic plaques in patients using optical coherence tomography: comparison with intravascular ultrasound.J Am Coll Cardiol. 2002 Feb 20;39(4):604-9. doi: 10.1016/s0735-1097(01)01799-5. J Am Coll Cardiol. 2002. PMID: 11849858 Clinical Trial.
-
Optical Coherence Tomography to Evaluate Plaque Burden and Morphology in Patients With Takotsubo Syndrome.J Am Heart Assoc. 2016 Dec 22;5(12):e004474. doi: 10.1161/JAHA.116.004474. J Am Heart Assoc. 2016. PMID: 28007746 Free PMC article.
-
A Survey on Coronary Atherosclerotic Plaque Tissue Characterization in Intravascular Optical Coherence Tomography.Curr Atheroscler Rep. 2018 May 21;20(7):33. doi: 10.1007/s11883-018-0736-8. Curr Atheroscler Rep. 2018. PMID: 29781047 Review.
-
Assessment of Coronary Plaque Vulnerability with Optical Coherence Tomography.Acta Cardiol Sin. 2014 Jan;30(1):1-9. Acta Cardiol Sin. 2014. PMID: 27122761 Free PMC article. Review.
References
-
- Knowles JW, Stone NJ, Ballantyne CM. Familial hypercholesterolemia and the 2013 American College of Cardiology/American Heart Association Guidelines: myths, oversimplification, and misinterpretation versus facts. Am J Cardiol. 2015;116:481–484. - PubMed
-
- Soutar AK, Naoumova RP. Mechanisms of disease: genetic causes of familial hypercholesterolemia. Nat Clin Pract Cardiovasc Med. 2007;4:214–225. - PubMed
-
- Watts G F, Gidding S, Wierzbicki A S, et al. Integrated guidance on the care of familial hypercholesterolaemia from the international FH foundation: executive summary. J Atheroscler Thromb. 2014;21:368–374. - PubMed
-
- Kume T, Akasaka T, Kawamoto T, et al. Measurement of the thickness of the fibrous cap by optical coherence tomography. Am Heart J. 2006;152:755.e1–755.e4. - PubMed
-
- Sinclair H, Bourantas C, Bagnall A, et al. OCT for the identification of vulnerable plaque in acute coronary syndrome. JACC Cardiovasc Imaging. 2015;8:198–209. - PubMed
LinkOut - more resources
Full Text Sources