

Dermatomyositis associated with omalizumab therapy for severe asthma: a case report
- PMID: 30675173
- PMCID: PMC6337756
- DOI: 10.1186/s13223-019-0319-4
Dermatomyositis associated with omalizumab therapy for severe asthma: a case report
Abstract
Background: Omalizumab is a humanized monoclonal antibody widely used for treatment of persistent allergic asthma and antihistamine-refractory chronic urticaria. Immediate adverse events to omalizumab are well characterized. Delayed anaphylactoid and serum sickness-like reactions have also been described; however, their relationship to the drug remains uncertain, and the frequency is unknown.
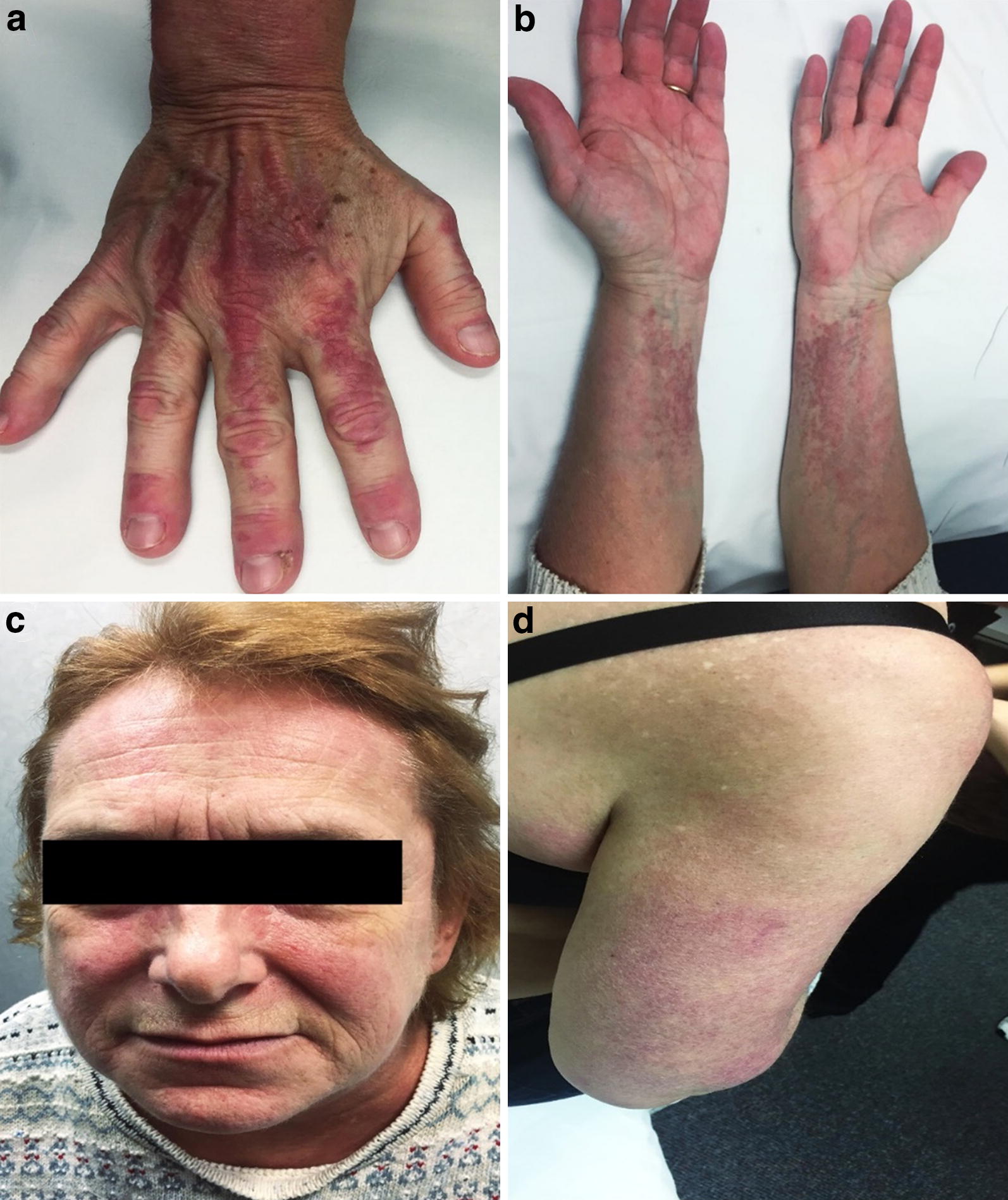
Case presentation: We present a case of a 59-year old female who developed amyopathic dermatomyositis (DM) after receiving omalizumab infusions for steroid-refractory severe asthma. After 6 months of omalizumab, the patient developed an erythematous, intensely pruritic cutaneous eruption. Skin biopsy indicated nonspecific features of dermatitis. However, neither topical corticosteroids nor gabapentin and maximal doses of multiple antihistamines gave her relief. On follow-up clinical exam 8 months later, she had classic cutaneous features of dermatomyositis, with confirmatory repeat skin biopsy. Laboratory investigations revealed negative myositis specific antibodies, positive antinuclear antibody, and negative anti-histone antibodies. Creatine kinase, lactate dehydrogenase, aspartate aminotransferase, alanine aminotransferase levels and C-reactive protein were also within normal limits. These findings supported the clinical impression of amyopathic DM. The patient's symptoms improved with oral corticosteroid therapy. A malignancy screen was negative. There was no evidence of end organ dysfunction.
Conclusions: Dermatomyositis is not a known adverse effect of omalizumab therapy. DM has a low incidence, but potentially life threatening consequences. Amyopathic DM may represent up to 21% of cases of DM, with similar risks of malignancy and end organ dysfunction. DM has been associated with biologic therapy. Using the Naranjo adverse drug reaction (ADR) probability scale, our patient had a "probable" omalizumab related ADR. A more likely explanation is that the patient had underlying DM that remained occult due to chronic corticosteroid therapy. Our case highlights the need for clinical vigilance and maintenance of a broad differential when patients on biologic therapies present with cutaneous eruptions. In our patient, the cutaneous clinical features of DM became pronounced over serial assessments. Laboratory markers may be deceptively normal, as in amyotrophic DM, or confounded by ongoing corticosteroid therapy. There are important clinical implications of prompt diagnosis, given the association of DM with end organ disease including interstitial lung disease, and possible concomitant malignancy.
Keywords: Adverse drug reaction; Biologics; Dermatomyositis; Omalizumab.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
