

Subscapularis tears: hidden and forgotten no more
- PMID: 30675571
- PMCID: PMC6334875
- DOI: 10.1016/j.jses.2017.11.006
Subscapularis tears: hidden and forgotten no more
Abstract
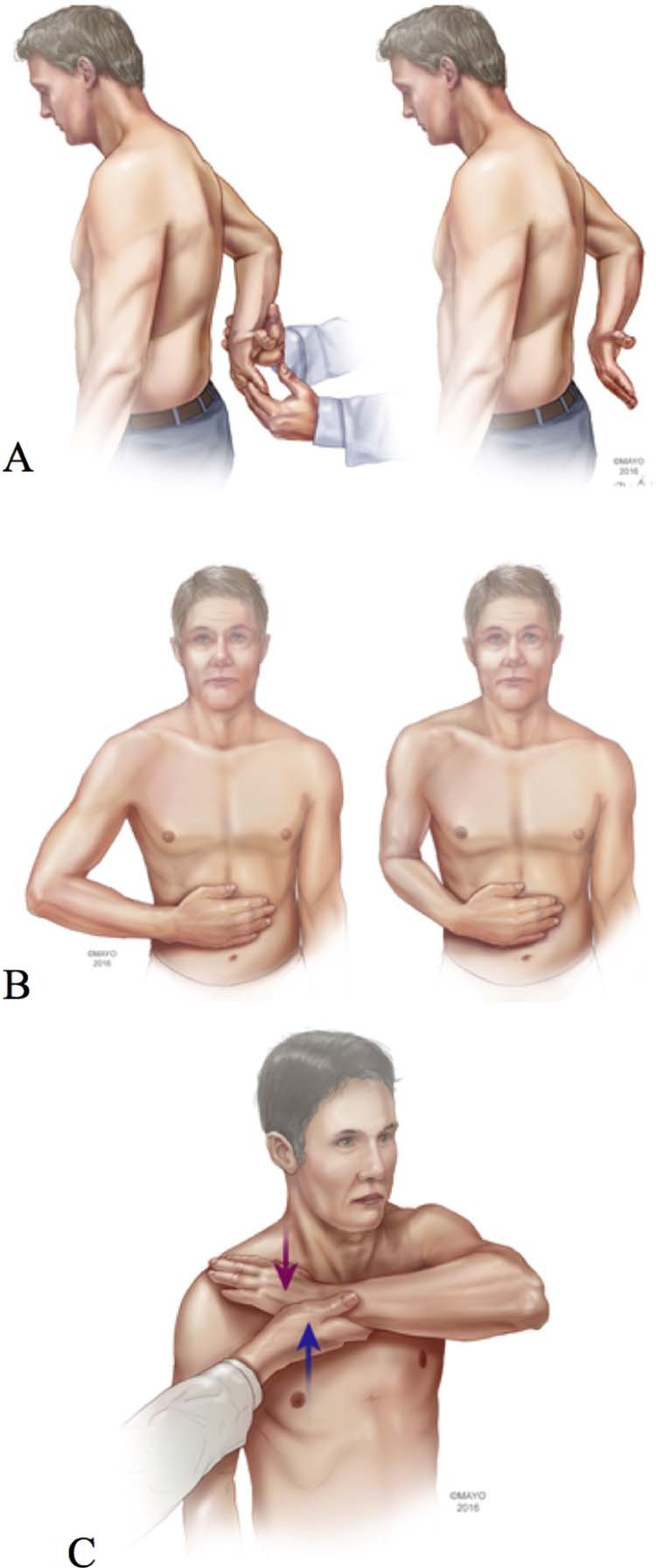
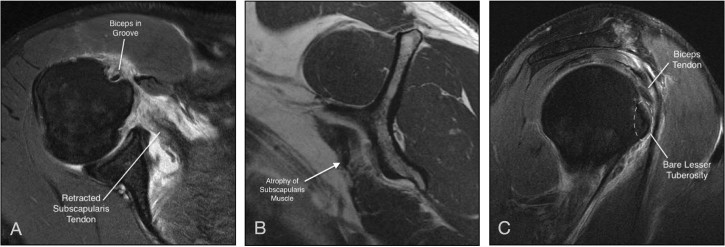
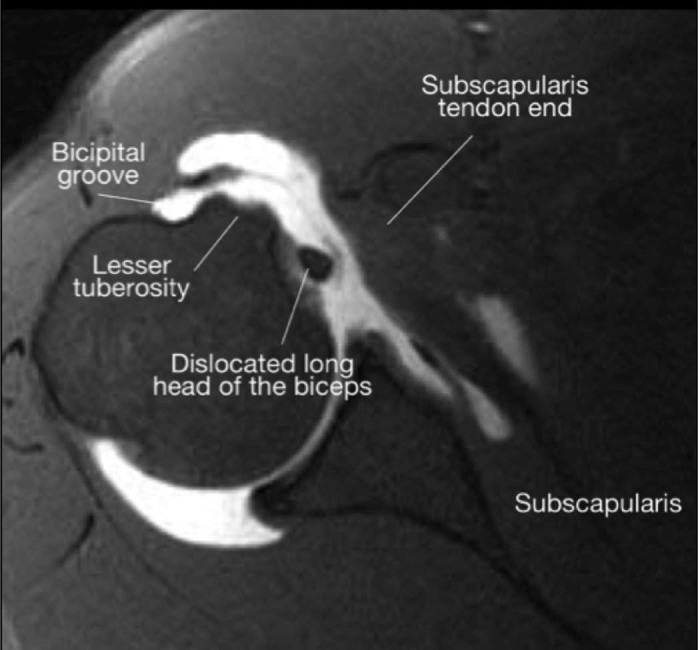
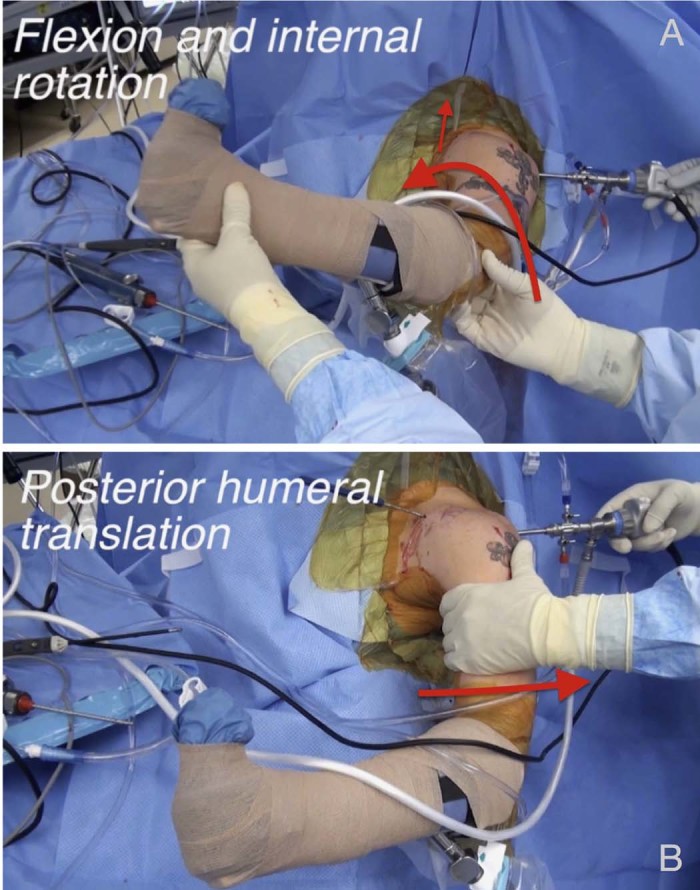
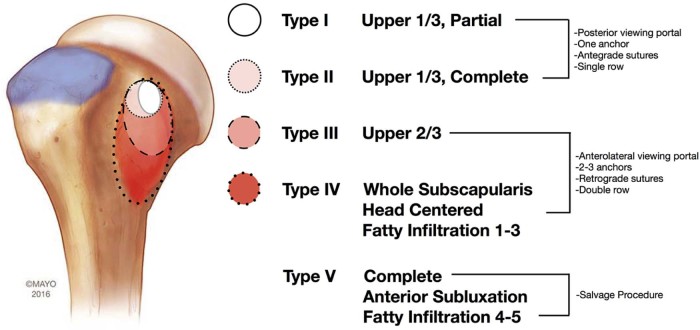
The subscapularis tendon, at one point, was thought of as the forgotten tendon, with "hidden lesions" that referred to partial tears of this tendon. Better understanding of anatomy and biomechanics combined with improved imaging technology and the widespread use of arthroscopy has led to a higher rate of subscapularis tear diagnoses and repairs. The bulk mass of the subscapularis muscle is more than that of all 3 other rotator cuff muscles combined. It functions as the internal rotator of the shoulder as the stout, rolled border of its tendon inserts onto the superior portion of the lesser tuberosity. A thorough history combined with specific physical examination maneuvers (including the bear hug, lift-off, and belly-press tests) is critical for accurate diagnosis. A systematic approach to advanced shoulder imaging also improves diagnostic capacity. Once identified, most subscapularis tendon tears can be successfully repaired arthroscopically. The Lafosse classification is useful as part of a treatment algorithm. Type I and II tears may be addressed while viewing from the standard posterior glenohumeral portal; larger Lafosse type III and IV tears are best repaired with anterior visualization at the subacromial or subdeltoid space. Tendon mobilization for larger tears is critical for adequate repair. In Lafosse type V tears, in which there is glenohumeral imbalance, tendon transfers and reverse replacement are commonly considered salvage options.
Keywords: Arthroscopic rotator cuff repair; Irreparable subscapularis; Rotator cuff imaging; Rotator cuff tear; Shoulder tendon transfer; Subscapularis physical examination; Subscapularis tear.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
