

Characteristics and Outcomes of Critical Illness in Children With Feeding and Respiratory Technology Dependence
- PMID: 30676492
- PMCID: PMC6502673
- DOI: 10.1097/PCC.0000000000001868
Characteristics and Outcomes of Critical Illness in Children With Feeding and Respiratory Technology Dependence
Abstract
Objectives: Children with dependence on respiratory or feeding technologies are frequently admitted to the PICU, but little is known about their characteristics or outcomes. We hypothesized that they are at increased risk of critical illness-related morbidity and mortality compared with children without technology dependence.
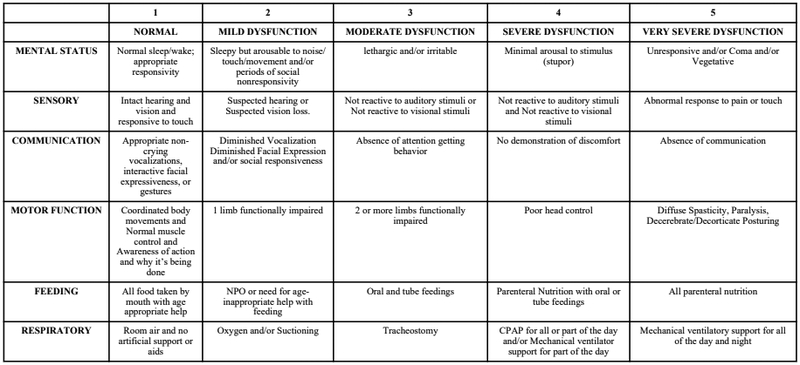
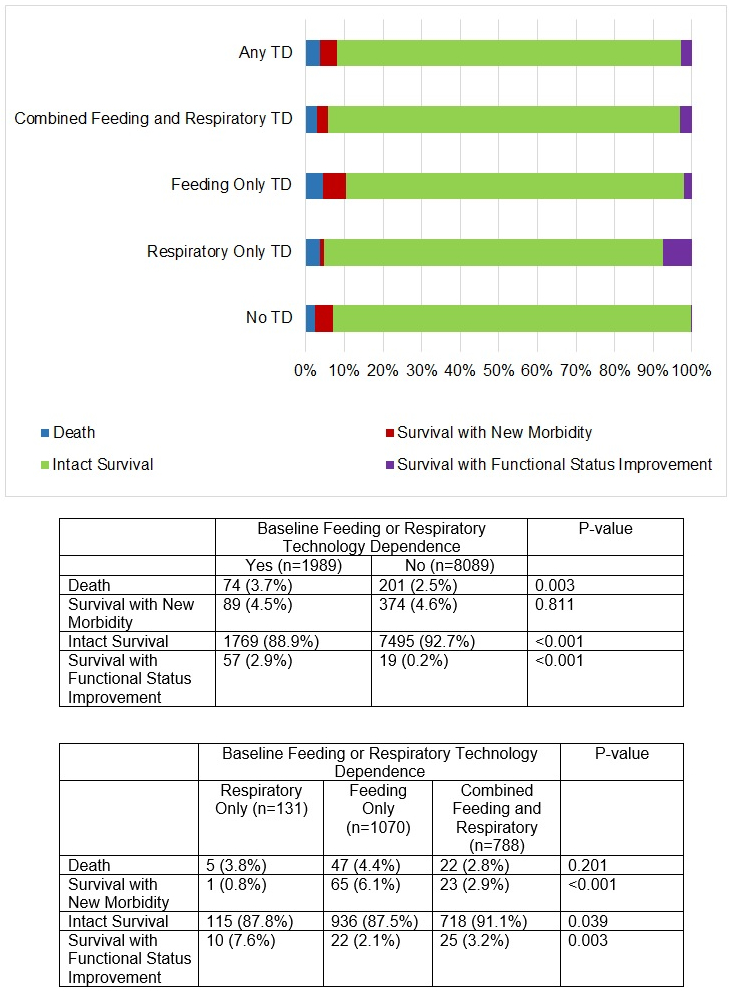
Design: Secondary analysis of prospective, probability-sampled cohort study of children from birth to 18 years old. Demographic and clinical characteristics were assessed. Outcomes included death, survival with new morbidity, intact survival, and survival with functional status improvement.
Setting: General and cardiovascular PICUs at seven participating children's hospitals as part of the Trichotomous Outcome Prediction in Critical Care study.
Subjects: Children from birth to 18 years of age as part of the Trichotomous Outcome Prediction in Critical Care study.
Interventions: None.
Measurements and main results: Children with technology dependence composed 19.7% (1,989/10,078) of PICU admissions. Compared with those without these forms of technology dependence, these children were younger, received more ICU-specific therapeutics, and were more frequently readmitted to the ICU. Death occurred in 3.7% of technology-dependent patients (n = 74), and new morbidities developed in 4.5% (n = 89). Technology-dependent children who developed new morbidities had higher Pediatric Risk of Mortality scores and received more ICU therapies than those who did not. A total of 3.0% of technology-dependent survivors (n = 57) showed improved functional status at hospital discharge.
Conclusions: Children with feeding and respiratory technology dependence composed approximately 20% of PICU admissions. Their new morbidity rates are similar to those without technology dependence, which contradicts our hypothesis that children with technology dependence would demonstrate worse outcomes. These comparable outcomes, however, were achieved with additional resources, including the use of more ICU therapies and longer lengths of stay. Improvement in functional status was seen in some technology-dependent survivors of critical illness.
Figures
References
-
- Ralston SL, Harrison W, Wasserman J, et al. Hospital variation in health care utilization by children with medical complexity. Pediatrics. 2015; 136(5):860–867. - PubMed
-
- Dosa N, Boeing N, Kanter R. Excess risk of severe acute Illness in children with chronic health conditions. Pediatrics. 2001; 107(3):499–504. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- Z99 HD999999/ImNIH/Intramural NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
