

Flexion Instability After Total Knee Arthroplasty
- PMID: 30676514
- PMCID: PMC6938456
- DOI: 10.5435/JAAOS-D-18-00347
Flexion Instability After Total Knee Arthroplasty
Abstract
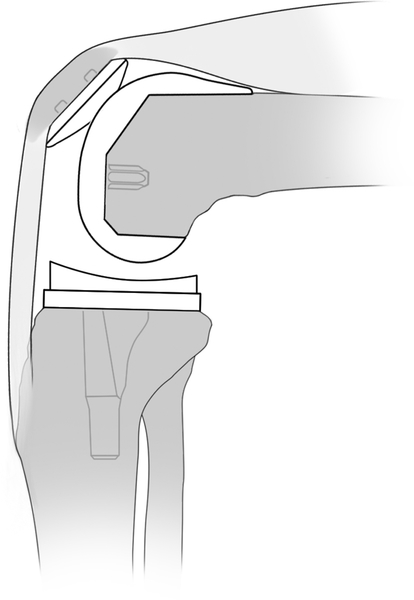
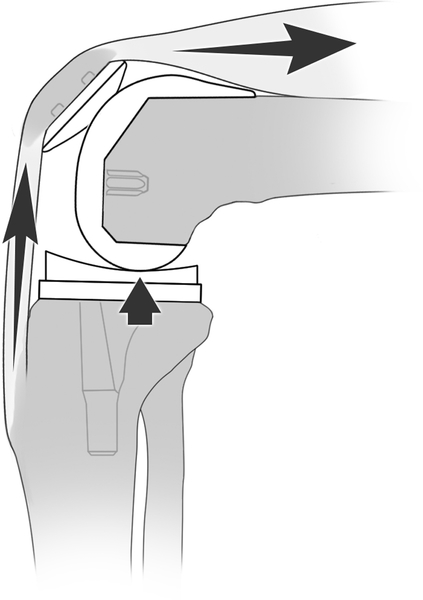
Flexion instability after total knee arthroplasty (TKA) is caused by an increased flexion gap compared with extension gap. Patients present with recurrent effusions, subjective instability (especially going downstairs), quadriceps weakness, and diffuse periretinacular pain. Manual testing for laxity in flexion is commonly done to confirm a diagnosis, although testing positions and laxity grades are inconsistent. Nonsurgical treatment includes quadriceps strengthening and bracing treatment. The mainstays to surgical management of femoral instability involve increasing the posterior condylar offset, decreasing the tibial slope, raising the joint line in combination with a thicker polyethylene insert, and ensuring appropriate rotation of implants. Patient outcomes after revision TKA for flexion instability show the least amount of improvement when compared with revisions for other TKA failure etiologies. Future work is needed to unify reproducible diagnostic criteria. Advancements in biomechanical analysis with motion detection, isokinetic quadriceps strength testing, and computational modeling are needed to advance the collective understanding of this underappreciated failure mechanism.
Figures









References
-
- Sharkey PF, Lichstein PM, Shen C, Tokarski AT, Parvizi J. Why Are Total Knee Arthroplasties Failing Today—Has Anything Changed After 10 Years? J Arthroplasty. 2014;29(9):1774–1778. - PubMed
-
- Dalury DF, Pomeroy DL, Gorab RS, Adams MJ. Why are Total Knee Arthroplasties Being Revised? J Arthroplasty. 2013;28(8):120–121. - PubMed
-
- Cottino U, Sculco PK, Sierra RJ, Abdel MP. Instability After Total Knee Arthroplasty. Orthop Clin North Am. 2016;47(2):311–316. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
