

Efficacy and Safety of Avelumab for Patients With Recurrent or Refractory Ovarian Cancer: Phase 1b Results From the JAVELIN Solid Tumor Trial
- PMID: 30676622
- PMCID: PMC6439837
- DOI: 10.1001/jamaoncol.2018.6258
Efficacy and Safety of Avelumab for Patients With Recurrent or Refractory Ovarian Cancer: Phase 1b Results From the JAVELIN Solid Tumor Trial
Abstract
Importance: Current treatment options for progressive ovarian cancer provide limited benefit, particularly in patients whose disease has become resistant to platinum-based chemotherapy.
Objective: To assess the efficacy and safety of avelumab, an anti-programmed death-ligand 1 agent, in a cohort of patients with previously treated recurrent or refractory ovarian cancer.
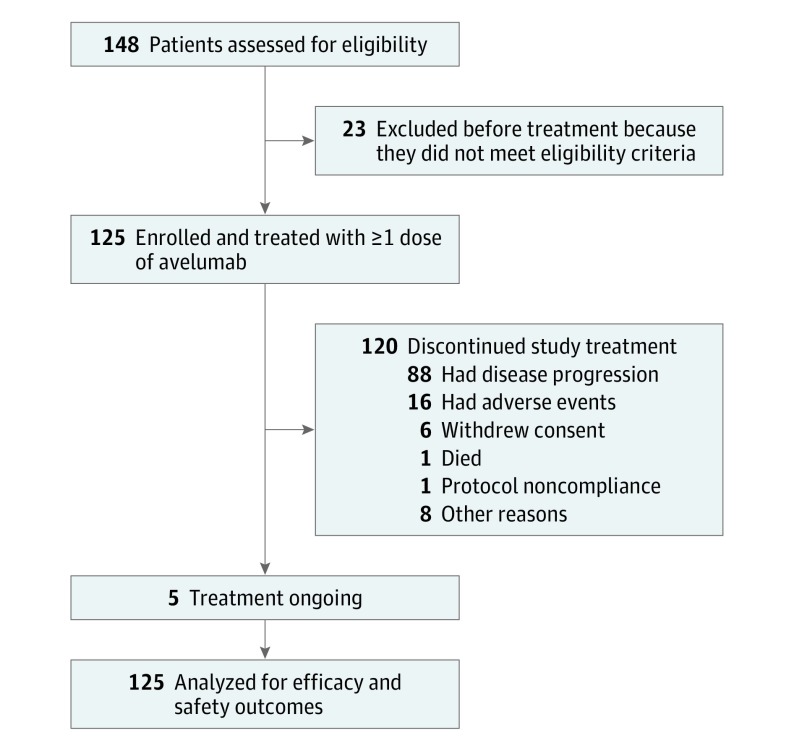
Design, setting, and participants: In an expansion cohort of a phase 1b, open-label study (JAVELIN Solid Tumor), 125 patients with advanced ovarian cancer who had received chemotherapy including a platinum agent were enrolled between November 6, 2013, and August 27, 2015. Statistical analysis was performed from December 31, 2016, to October 9, 2018.
Intervention: Patients received avelumab, 10 mg/kg, every 2 weeks until disease progression, unacceptable toxic effects, or withdrawal from the study.
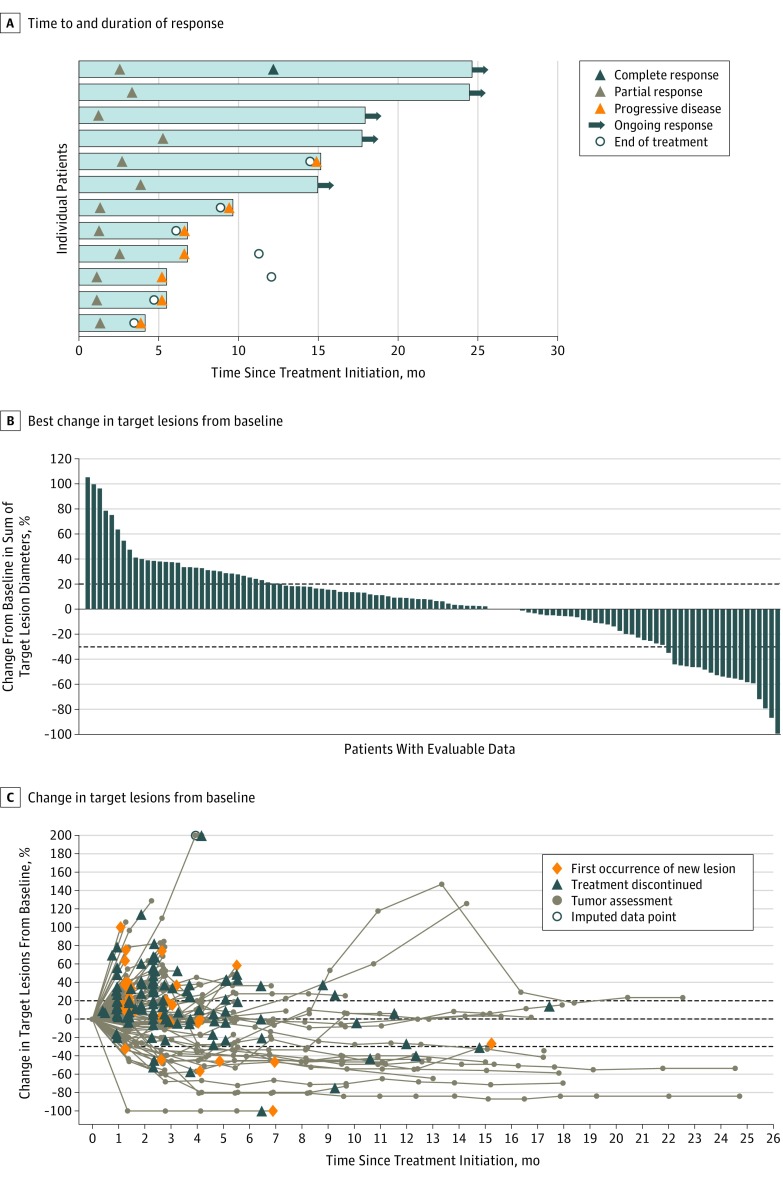
Main outcomes and measures: Prespecified end points in this cohort included confirmed best overall response (per Response Evaluation Criteria In Solid Tumors, version 1.1), immune-related best overall response, duration of response, progression-free survival, overall survival, results of programmed death-ligand 1 expression-based analyses, and safety.
Results: A total of 125 women (median age, 62.0 years [range, 27-84 years]) who had received a median of 3 prior lines of treatment (range, 0-10) for advanced disease were enrolled in the study. Patients received avelumab for a median of 2.8 months (range, 0.5-27.4 months), with a median follow-up of 26.6 months (range, 16-38 months). A confirmed objective response occurred in 12 patients (9.6%; 95% CI, 5.1%-16.2%), including a complete response in 1 patient (0.8%) and a partial response in 11 patients (8.8%). The 1-year progression-free survival rate was 10.2% (95% CI, 5.4%-16.7%) and median overall survival was 11.2 months (95% CI, 8.7-15.4 months). Infusion-related reactions occurred in 25 patients (20.0%). Other frequent treatment-related adverse events (any grade event occurring in ≥10% of patients) were fatigue (17 [13.6%]), diarrhea (15 [12.0%]), and nausea (14 [11.2%]). Grade 3 or higher treatment-related adverse events occurred in 9 patients (7.2%), of which only the level of lipase increased (3 [2.4%]) occurred in more than 1 patient. Twenty-one patients (16.8%) had an immune-related adverse event of any grade. No treatment-related deaths occurred.
Conclusions and relevance: Avelumab demonstrated antitumor activity and acceptable safety in heavily pretreated patients with recurrent or refractory ovarian cancer.
Trial registration: ClinicalTrials.gov identifier: NCT01772004.
Conflict of interest statement
Figures
References
-
- National Comprehensive Cancer Network NCCN clinical practice guidelines in oncology: ovarian cancer. V2.2018. https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf. Accessed September 20, 2018.
