

An optimized low-pressure tourniquet murine hind limb ischemia reperfusion model: Inducing acute ischemia reperfusion injury in C57BL/6 wild type mice
- PMID: 30677066
- PMCID: PMC6345480
- DOI: 10.1371/journal.pone.0210961
An optimized low-pressure tourniquet murine hind limb ischemia reperfusion model: Inducing acute ischemia reperfusion injury in C57BL/6 wild type mice
Abstract
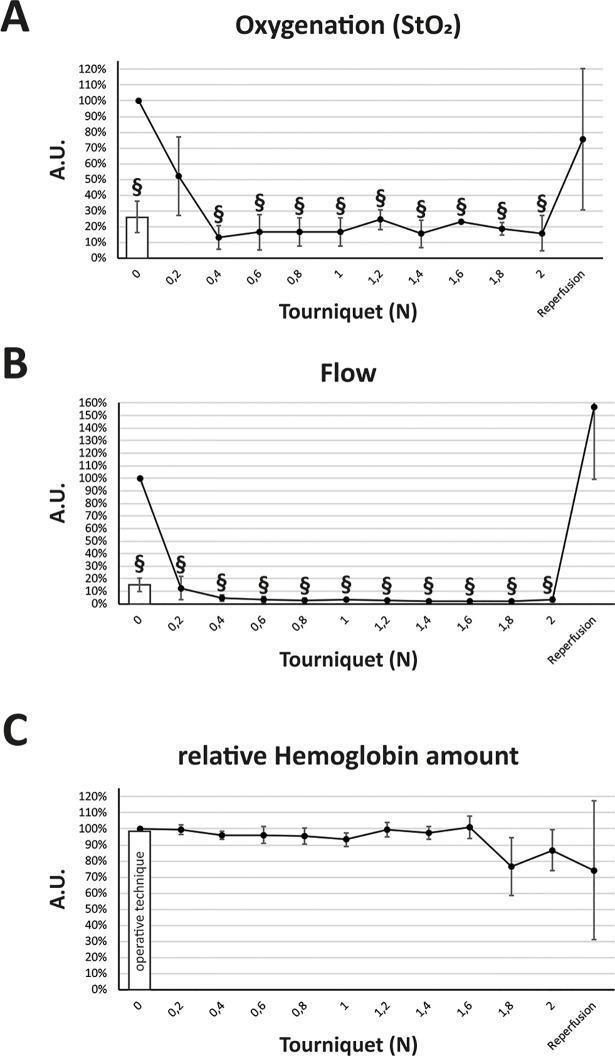
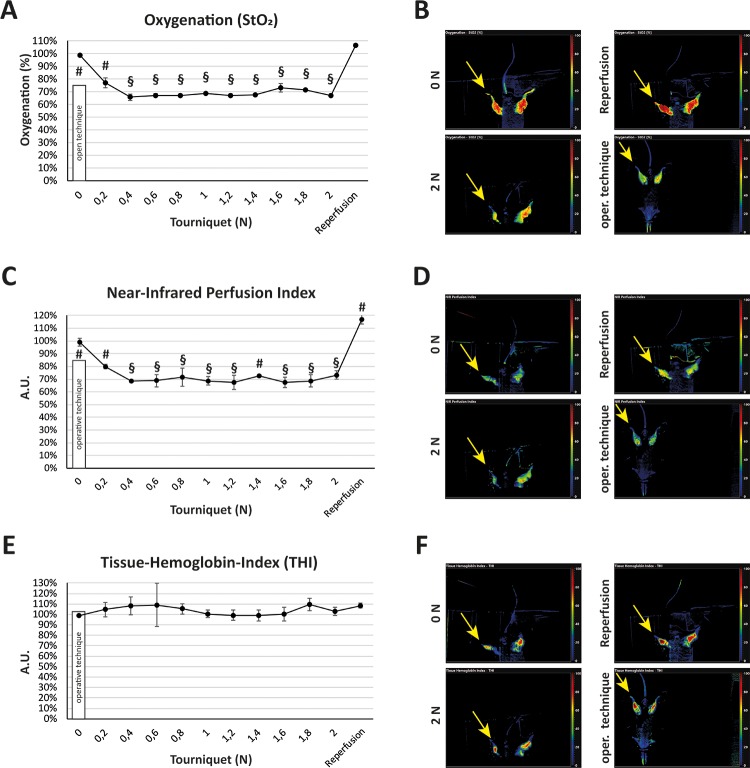
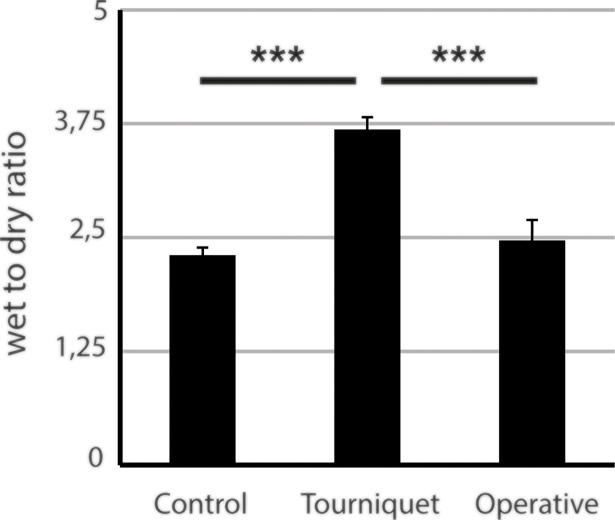
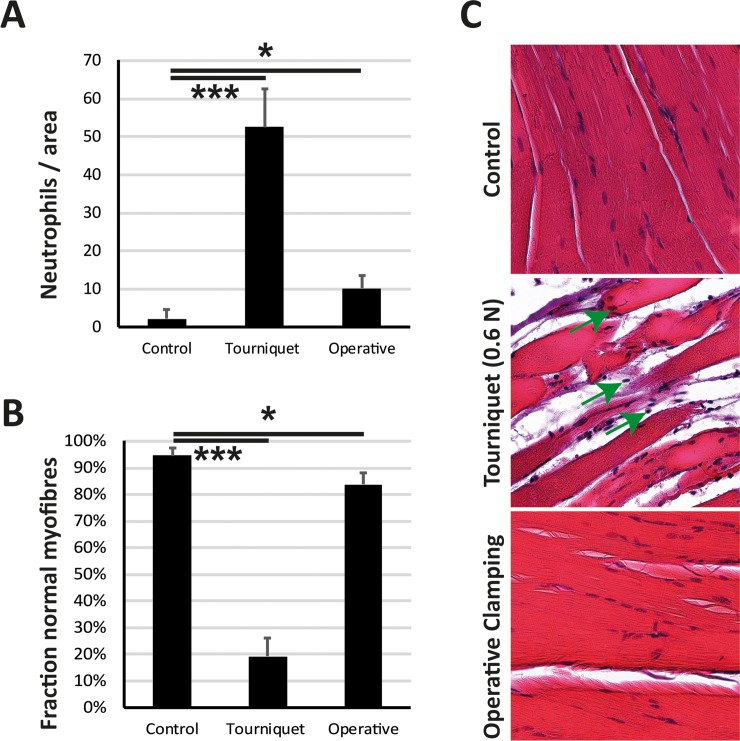
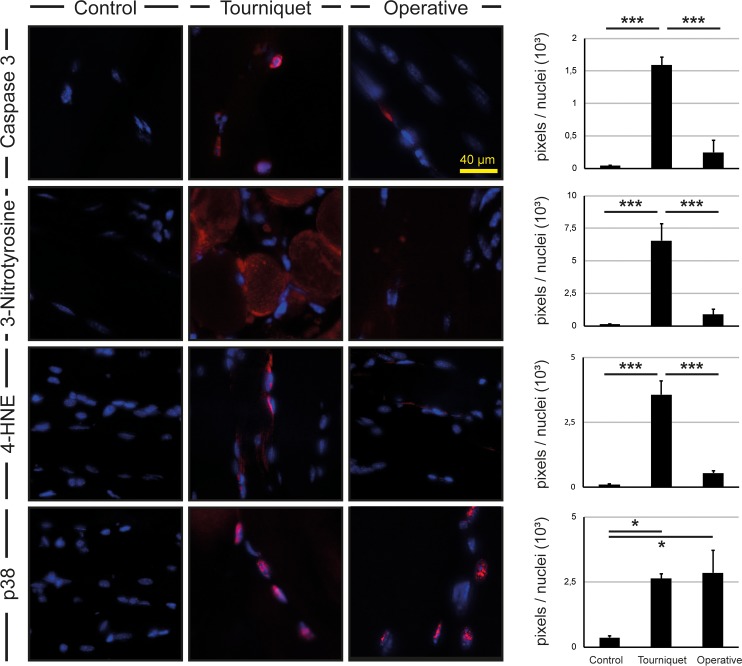
Acute ischemia reperfusion injury in skeletal muscle remains an important issue in several fields of regenerative medicine. Thus, a valid model is essential to gain deeper insights into pathophysiological relations and evaluate possible treatment options. While the vascular anatomy of mice regularly prevents sufficient vessel occlusion by invasive methods, there is a multitude of existing models to induce ischemia reperfusion injury without surgical procedures. Since there is no consensus on which model to prefer, this study aims to develop and evaluate a novel, optimized low-pressure tourniquet model. C57BL/6 mice underwent an ischemic procedure by either tourniquet or invasive artery clamping. A sham group served as control. With exception of the sham group, mice underwent 2 hours of ischemia followed by 4 hours of reperfusion. Groups were compared using microcirculatory and spectroscopic measurements, distinctions in tissue edema, histological and immunohistochemical analyses. Both procedures led to a significant decrease in tissue blood flow (- 97% vs. - 86%) and oxygenation (- 87% vs. - 75%) with a superiority of the low-pressure tourniquet. Tissue edema in the tourniquet cohort was significantly increased (+ 59%), while the increase in the clamping cohort was non-significant (+ 7%). Haematoxylin Eosin staining showed significantly more impaired muscle fibers in the tourniquet group (+ 77 p.p. vs. + 11 p.p.) and increased neutrophil infiltration/ROI (+ 51 vs. + 8). Immunofluorescence demonstrated an equal increase of p38 in both groups (7-fold vs. 8-fold), while the increase in apoptotic markers (Caspase-3, 3-Nitrotyrosine, 4-Hydroxynonenal) was significantly higher in the tourniquet group. The low-pressure tourniquet has been proven to produce reproducible and thus reliable ischemia reperfusion injury. In addition, significantly less force was needed than previously stated. It is therefore an important instrument for studying the pathophysiology of ischemia reperfusion injury and for the development of prophylactic as well as therapeutic interventions.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Weiskopf RB, Collard CD, Gelman S. Pathophysiology, Clinical Manifestations, and Prevention of Ischemia–Reperfusion Injury Basic Pathophysiology of Ischemia–Reperfusion Injury. Anesthesiology. 2001;94: 1133–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
