

Polypharmacy in outpatients with relapsing-remitting multiple sclerosis: A single-center study
- PMID: 30677078
- PMCID: PMC6345436
- DOI: 10.1371/journal.pone.0211120
Polypharmacy in outpatients with relapsing-remitting multiple sclerosis: A single-center study
Abstract
Background: Multiple sclerosis (MS) is an immune-mediated disease of the central nervous system. Given the chronic and heterogenous nature of the disease, treatment with various therapies is a frequent scenario in clinical practice. In persons with chronic morbidity such as MS patients, polypharmacy can give rise to considerable health problems.
Objectives: The aim of the present study was to examine the frequency of polypharmacy among relapsing-remitting (RR) MS patients as well as to analyse sociodemographic and clinical factors, which might be associated with polypharmacy (use of five or more medications). Differences in medication between MS patients with and without secondary illnesses (PwSI and Pw/oSI), between men and women and between patients with and without polypharmacy (PwP and Pw/oP) were examined.
Methods: For 145 RRMS outpatients, we prospectively collected data by means of anamnesis, patient records, clinical examination and a structured patient interview. This was followed by comparative analyses of various patient subgroups (PwP vs. Pw/oP, PwSI vs. Pw/oSI, men vs. women).
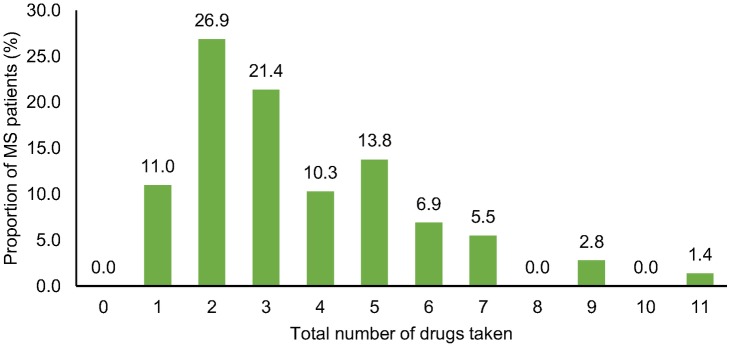
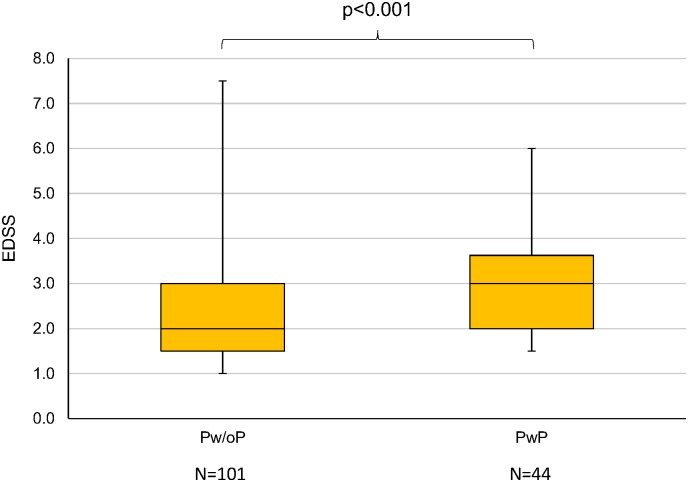
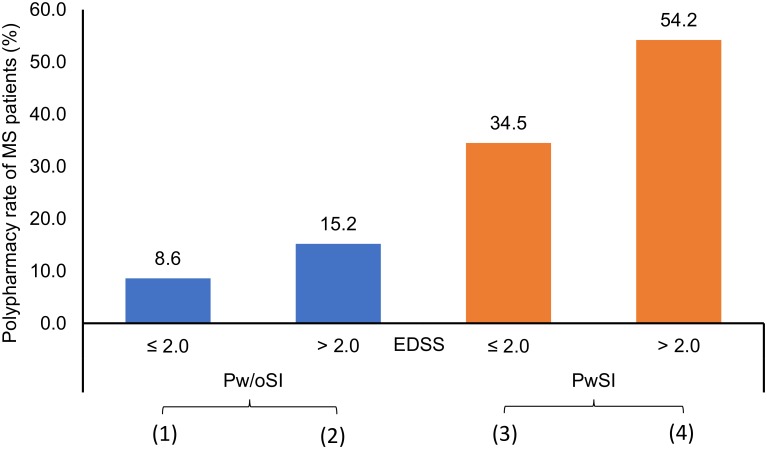
Results: The proportion of included MS patients with polypharmacy (use of ≥5 medications) was 30.3%. PwP were significantly older than Pw/oP (45.9 vs. 41.7 years), had a lower level of education and showed a significantly higher median EDSS score (3.0 vs. 2.0). Comorbidities (p<0.001; odds ratio [OR] = 6.293) and higher EDSS scores (p = 0.029; OR = 1.440) were associated with a higher risk of polypharmacy. The proportion of polypharmacy among PwSI was approximately four times higher than among Pw/oSI (46.8% vs. 11.8%). Particularly in the use of antihypertensives, gastrointestinal drugs and dietary supplements, there were differences between Pw/oP and PwP.
Conclusion: We found a high burden of polypharmacy in patients with RRMS. This particularly applies to more severely disabled MS patients who suffer from comorbidities.
Conflict of interest statement
MH received speaking fees and travel funds from Bayer HealthCare, Biogen, Novartis and Teva. UKZ received research support as well as speaking fees and travel funds from Almirall, Bayer HealthCare, Biogen, Merck Serono, Novartis, Sanofi and Teva. NF declares no competing interests. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Multi-drug use among patients with multiple sclerosis: A cross-sectional study of associations to clinicodemographic factors.Sci Rep. 2019 Mar 6;9(1):3743. doi: 10.1038/s41598-019-40283-5. Sci Rep. 2019. PMID: 30842515 Free PMC article.
-
Cognitive impairment and its relation with disease measures in mildly disabled patients with relapsing-remitting multiple sclerosis: baseline results from the Cognitive Impairment in Multiple Sclerosis (COGIMUS) study.Mult Scler. 2009 Jul;15(7):779-88. doi: 10.1177/1352458509105544. Mult Scler. 2009. PMID: 19542262
-
Mitoxantrone in relapsing-remitting and rapidly progressive multiple sclerosis: Ten-year clinical outcomes post-treatment with mitoxantrone.Mult Scler Relat Disord. 2020 Sep;44:102330. doi: 10.1016/j.msard.2020.102330. Epub 2020 Jun 23. Mult Scler Relat Disord. 2020. PMID: 32599468
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
Management of worsening multiple sclerosis with mitoxantrone: a review.Clin Ther. 2006 Apr;28(4):461-74. doi: 10.1016/j.clinthera.2006.04.013. Clin Ther. 2006. PMID: 16750460 Review.
Cited by
-
Polypharmacy in patients with multiple sclerosis and the impact on levels of care and therapy units.Front Neurol. 2023 Dec 21;14:1330066. doi: 10.3389/fneur.2023.1330066. eCollection 2023. Front Neurol. 2023. PMID: 38187151 Free PMC article.
-
Cardiac Autonomic Dysfunction in Multiple Sclerosis: A Systematic Review of Current Knowledge and Impact of Immunotherapies.J Clin Med. 2020 Jan 24;9(2):335. doi: 10.3390/jcm9020335. J Clin Med. 2020. PMID: 31991711 Free PMC article. Review.
-
Clinical characteristics of middle-aged and older patients with MS treated with interferon beta-1b: post-hoc analysis of a 2-year, prospective, international, observational study.BMC Neurol. 2021 Aug 23;21(1):324. doi: 10.1186/s12883-021-02347-w. BMC Neurol. 2021. PMID: 34425763 Free PMC article.
-
Personality traits in patients with multiple sclerosis: their association with nicotine dependence and polypharmacy.Ther Adv Neurol Disord. 2024 Oct 14;17:17562864241279118. doi: 10.1177/17562864241279118. eCollection 2024. Ther Adv Neurol Disord. 2024. PMID: 39411724 Free PMC article.
-
Polypharmacy in Multiple Sclerosis: Current Knowledge and Future Directions.Mo Med. 2021 May-Jun;118(3):239-245. Mo Med. 2021. PMID: 34149084 Free PMC article.
References
-
- Gilmour H, Ramage-Morin PL, Wong SL. Multiple sclerosis. Prevalence and impact. Health Rep. 2018;29: 3–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
