

Readmission and hospital mortality after ICU discharge of critically ill cancer patients
- PMID: 30677085
- PMCID: PMC6345475
- DOI: 10.1371/journal.pone.0211240
Readmission and hospital mortality after ICU discharge of critically ill cancer patients
Erratum in
-
Correction: Readmission and hospital mortality after ICU discharge of critically ill cancer patients.PLoS One. 2019 Jun 5;14(6):e0218196. doi: 10.1371/journal.pone.0218196. eCollection 2019. PLoS One. 2019. PMID: 31167000 Free PMC article.
Abstract
Background: Intensive care unit (ICU) readmission is generally associated with increased hospital stays and increased mortality. However, there are limited data on ICU readmission in critically ill cancer patients.
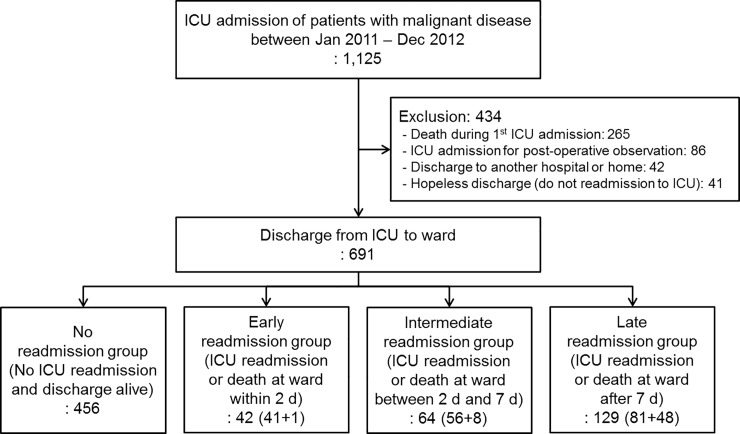
Method: We conducted a retrospective cohort study based on the prospective registry of all critically ill cancer patients admitted to the oncology medical ICU between January 2012 and December 2013. After excluding patients who were discharged to another hospital or decided to end-of-life care, we divided the enrolled patients into four groups according to the time period from ICU discharge to unexpected events (ICU readmission or ward death) as follows: no (without ICU readmission or death, n = 456), early (within 2 days, n = 42), intermediate (between 2 and 7 days, n = 64), and late event groups (after 7 days of index ICU discharge, n = 129). The independent risk factors associated with ICU readmission or unexpected death after ICU discharge were also analyzed using multinomial logistic regression model.
Results: There were no differences in the reasons for ICU readmission across the groups. ICU mortality did not differ among the groups, but hospital mortality was significantly higher in the late event group than in the early event group. Mechanical ventilation during ICU stay, tachycardia, decreased mental status, and thrombocytopenia on the day of index ICU discharge increased the risk of early ICU readmission or unexpected ward death, while admission through the emergency room and sepsis and respiratory failure as the reasons for index ICU admission were associated with increased risk of late readmission or unexpected ward death. Interestingly, recent chemotherapy within 4 weeks before index ICU admission was inversely associated with the risk of late readmission or unexpected ward death.
Conclusion: In critically ill cancer patients, patient characteristics predicting ICU readmission or unexpected ward death were different according to the time period between index ICU discharge and the events.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Does the implementation of a novel intensive care discharge risk score and nurse-led inpatient review tool improve outcome? A prospective cohort study in two intensive care units in the UK.BMJ Open. 2017 Dec 26;7(12):e018322. doi: 10.1136/bmjopen-2017-018322. BMJ Open. 2017. PMID: 29282265 Free PMC article.
-
Assessment of the Safety of Discharging Select Patients Directly Home From the Intensive Care Unit: A Multicenter Population-Based Cohort Study.JAMA Intern Med. 2018 Oct 1;178(10):1390-1399. doi: 10.1001/jamainternmed.2018.3675. JAMA Intern Med. 2018. PMID: 30128550 Free PMC article.
-
Readmission to the Intensive Care Unit: Incidence, Risk Factors, Resource Use, and Outcomes. A Retrospective Cohort Study.Ann Am Thorac Soc. 2017 Aug;14(8):1312-1319. doi: 10.1513/AnnalsATS.201611-851OC. Ann Am Thorac Soc. 2017. PMID: 28530118
-
A meta-analysis to derive literature-based benchmarks for readmission and hospital mortality after patient discharge from intensive care.Crit Care. 2014 Dec 31;18(6):715. doi: 10.1186/s13054-014-0715-6. Crit Care. 2014. PMID: 25551448 Free PMC article. Review.
-
Critical care transition programs on readmission or death: A systematic review and meta-analysis.Acta Anaesthesiol Scand. 2020 Aug;64(7):870-883. doi: 10.1111/aas.13591. Epub 2020 Apr 17. Acta Anaesthesiol Scand. 2020. PMID: 32232833
Cited by
-
Impact of Glasgow Coma Scale scores on unplanned intensive care unit readmissions among surgical patients.Ann Transl Med. 2019 Oct;7(20):520. doi: 10.21037/atm.2019.10.06. Ann Transl Med. 2019. PMID: 31807502 Free PMC article.
-
Vital Signs in Palliative Care: A Scoping Review.Cancers (Basel). 2023 Sep 20;15(18):4641. doi: 10.3390/cancers15184641. Cancers (Basel). 2023. PMID: 37760611 Free PMC article. Review.
-
Prognostic significance of albumin to alkaline phosphatase ratio in critically ill patients with acute kidney injury.Clin Exp Nephrol. 2022 Sep;26(9):917-924. doi: 10.1007/s10157-022-02234-9. Epub 2022 May 17. Clin Exp Nephrol. 2022. PMID: 35579723
-
Outcome of Cancer Patients with an Unplanned Intensive Care Unit Admission: Predictors of Mortality and Long-term Survival.Saudi J Med Med Sci. 2024 Apr-Jun;12(2):153-161. doi: 10.4103/sjmms.sjmms_145_23. Epub 2024 Apr 5. Saudi J Med Med Sci. 2024. PMID: 38764561 Free PMC article.
-
Nursing Activities Score at Discharge from the Intensive Care Unit Is Associated with Unplanned Readmission to the Intensive Care Unit.J Clin Med. 2022 Sep 2;11(17):5203. doi: 10.3390/jcm11175203. J Clin Med. 2022. PMID: 36079134 Free PMC article.
References
-
- Azoulay E, Mokart D, Pene F, Lambert J, Kouatchet A, Mayaux J, et al. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—a groupe de recherche respiratoire en reanimation onco-hematologique study. J Clin Oncol. 2013; 31:2810–8. 10.1200/JCO.2012.47.2365 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
