

Feasibility of a randomised controlled trial of remotely delivered problem-solving cognitive behaviour therapy versus usual care for young people with depression and repeat self-harm: lessons learnt (e-DASH)
- PMID: 30678674
- PMCID: PMC6346566
- DOI: 10.1186/s12888-018-2005-3
Feasibility of a randomised controlled trial of remotely delivered problem-solving cognitive behaviour therapy versus usual care for young people with depression and repeat self-harm: lessons learnt (e-DASH)
Abstract
Background: Self-harm and depression are strong risk factors for repeat self-harm and suicide. We aimed to investigate the feasibility of a randomised controlled trial (RCT) of remotely delivered problem-solving cognitive behaviour therapy (PSCBT) plus treatment as usual (TAU) versus TAU in young people with repeat self-harm and depression.
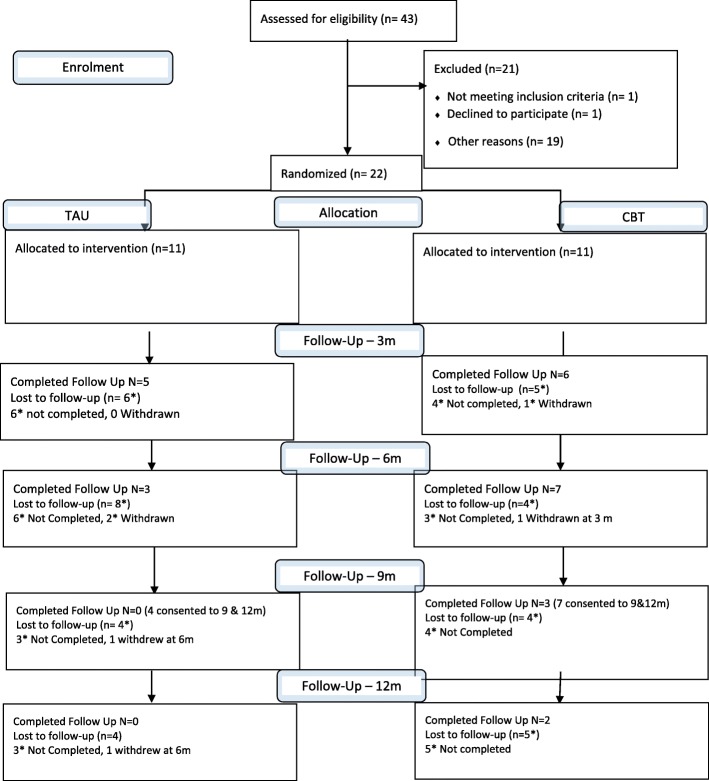
Methods: Single-blind multi-centre RCT with an internal pilot, pre-set stop-go criteria and qualitative semi-structured interviews. Eligible participants (aged 16-30 years) were recruited from 9 adult or child and adolescent self-harm and crisis services; had ≥ 2 lifetime self-harm episodes, one in the preceding 96 h; and Beck Depression Inventory-II (BDI-II) score ≥ 17. Participants were randomised (1:1) to either TAU or TAU and 10-12 sessions of PSCBT delivered by mobile phone or video-calling.
Results: Twenty-two participants were recruited (11 in each arm), 10 (46%) completed follow-up at 6 months, 9 (82%) started the PSCBT and 4 (36%) completed it. The study did not meet three of its four stop-go criteria, reflecting considerable barriers to recruitment and retention. Participants had severe depression symptoms: with mean BDI-II 38.9 in the PSCBT and 37.2 in TAU groups, respectively. Three (14%) unblindings occurred for immediate safety concerns. Barriers to recruitment and retention included lack of agency for participants, severity of depression, recency of crisis with burden for participants and clinicians who diagnosed depression according to pervasiveness.
Conclusions: RCTs of PSCBT for young people with depression and self-harm are not feasible using recruitment through mental health services that conduct assessments following self-harm presentations. Clinician assessment following self-harm presentation mainly identifies those with severe rather than mild-moderate depression.
Trial registration: ClinicalTrials.gov ( NCT02377011 ); Date of registration: March 3rd 2015. Retrospectively registered: within 21 days of recruitment of the first participant.
Keywords: Cognitive behaviour therapy; Depression; Problem-solving therapy; RCT; Self-harm.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the National Research Ethics Service (NRES) Committee East Midlands - Nottingham 1, UK on 24th September 2014 (REC reference: 14/EM/1084). All participants provided written informed consent. The consent included contact details of up to three family or close friend contacts that a participant was willing to give to the research team if there were safety concerns.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- National Institute for Health and Clinical Excellence. Self-harm: longer-term management. National Clinical Guideline Number 133. National Institute for Health and Clinical Excellence: London, 2012.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
