

Safety and efficacy of regional citrate anticoagulation for continuous renal replacement therapy in liver failure patients: a systematic review and meta-analysis
- PMID: 30678706
- PMCID: PMC6345001
- DOI: 10.1186/s13054-019-2317-9
Safety and efficacy of regional citrate anticoagulation for continuous renal replacement therapy in liver failure patients: a systematic review and meta-analysis
Abstract
Background: Regional citrate anticoagulation (RCA) is a widely used strategy for continuous renal replacement therapy (CRRT). Most of the current guidelines recommend liver failure as one of the contraindications for citrate anticoagulation. However, some studies suggested that the use of citrate for CRRT in liver failure patients did not increase the risk of citrate-related complications. The purpose of this systematic review is to summarize the current evidences on the safety and efficacy of RCA for CRRT in liver failure patients.
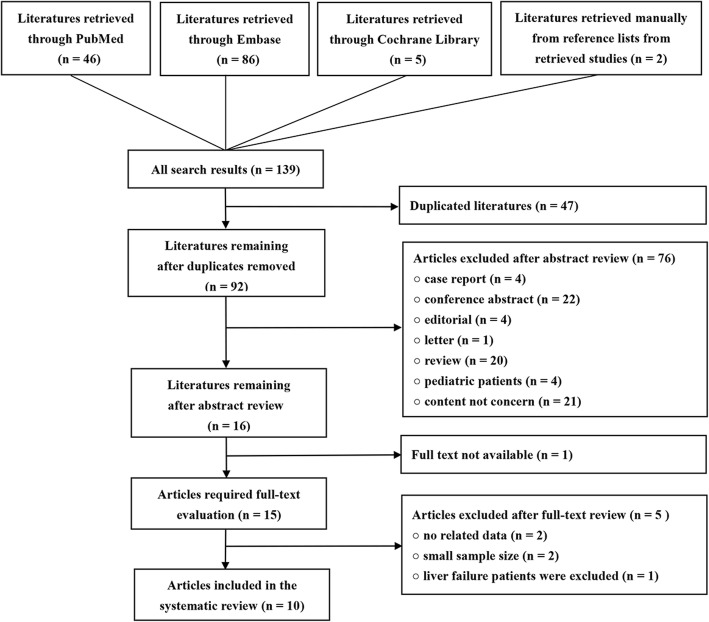
Methods: We performed a comprehensive search on PubMed, Embase, and the Cochrane Library databases from the inception to March 1, 2018. Studies enrolled adult (age > 18 years) patients with various levels of liver dysfunction underwent RCA-CRRT were included in this systematic review.
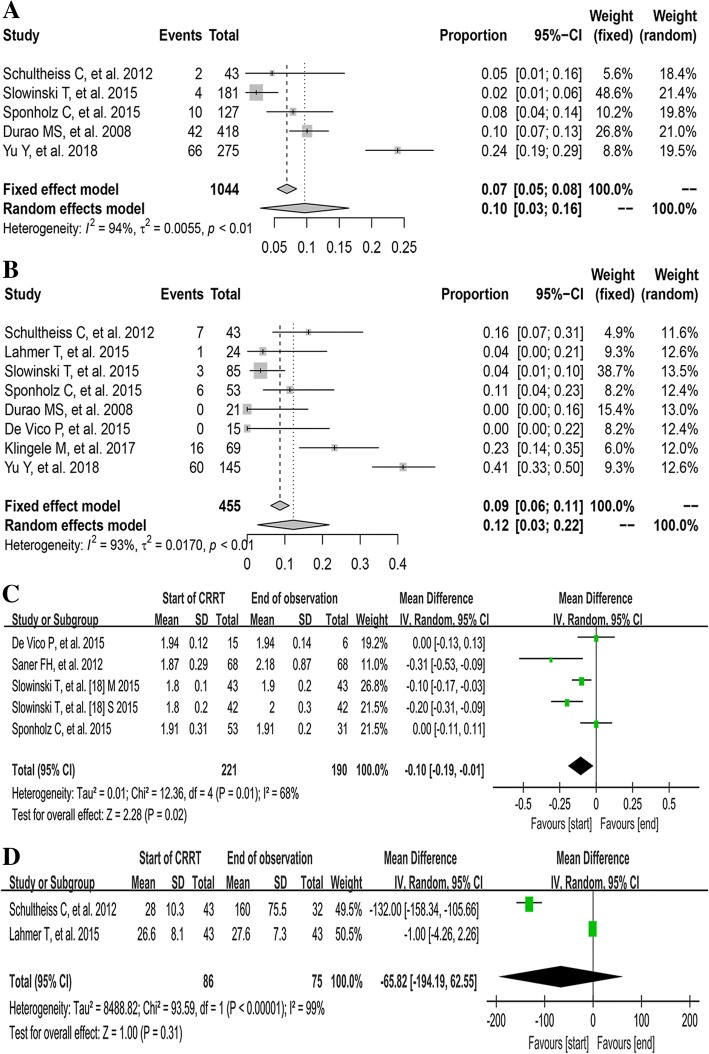
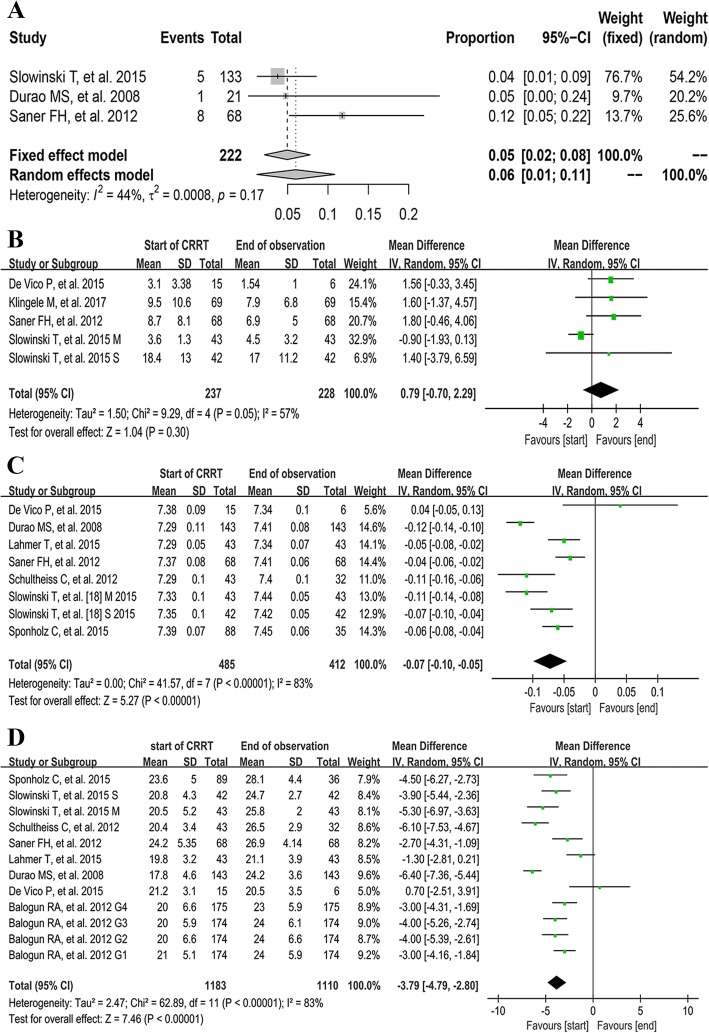
Results: After the study screening, 10 observational studies with 1241 liver dysfunction patients were included in this systematic review. The pooled rate of citrate accumulation and bleeding was 12% [3%, 22%] and 5% [2%, 8%], respectively. Compared with the baseline data, the serum pH, bicarbonate, and base excess (BE), the rate of metabolic alkalosis, the serum ionized calcium (ionCa) and total calcium (totCa) level, and the ratio of total calcium/ionized calcium (totCa/ionCa) significantly increased at the end of observation. However, no significant increase was observed in serum citrate (MD - 65.82 [- 194.19, 62.55]), lactate (MD 0.49 [- 0.27, 1.26]) and total bilirubin concentration (MD 0.79 [- 0.70, 2.29]) at the end of CRRT. Compared with non-liver failure patients, the live failure patients showed no significant difference in the pH (MD - 0.04 [- 0.13, 0.05]), serum lactate level (MD 0.69 [- 0.26, 1.64]), and totCa/ionCa ratio (MD 0.03 [- 0.12, 0.18]) during CRRT. The median of mean filter lifespan was 55.9 h, with a range from 22.7 to 72 h.
Conclusions: Regional citrate anticoagulation seems to be a safe anticoagulation method in liver failure patients underwent CRRT and could yield a favorable filter lifespan. Closely monitoring the acid base status and electrolyte balance may be more necessary during RCA-CRRT in patients with liver failure.
Keywords: Anticoagulation; Citrate; Continuous renal replacement therapy; Liver failure.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
In severe liver disease, citrate can be used safely: the question remains-by which mechanism.Crit Care. 2020 Feb 24;24(1):63. doi: 10.1186/s13054-020-2801-2. Crit Care. 2020. PMID: 32093726 Free PMC article. No abstract available.
References
-
- Liu C, Mao Z, Kang H, Hu J, Zhou F. Regional citrate versus heparin anticoagulation for continuous renal replacement therapy in critically ill patients: a meta-analysis with trial sequential analysis of randomized controlled trials. Crit Care. 2016;20:144. doi: 10.1186/s13054-016-1299-0. - DOI - PMC - PubMed
-
- Apsner R, Schwarzenhofer M, Derfler K, Zauner C, Ratheiser K, Kranz A. Impairment of citrate metabolism in acute hepatic failure. Wien Klin Wochenschr. 1997;109:123–127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
