

Spatial patterns of white matter hyperintensities associated with Alzheimer's disease risk factors in a cognitively healthy middle-aged cohort
- PMID: 30678723
- PMCID: PMC6346579
- DOI: 10.1186/s13195-018-0460-1
Spatial patterns of white matter hyperintensities associated with Alzheimer's disease risk factors in a cognitively healthy middle-aged cohort
Abstract
Background: White matter hyperintensities (WMH) of presumed vascular origin have been associated with an increased risk of Alzheimer's disease (AD). This study aims to describe the patterns of WMH associated with dementia risk estimates and individual risk factors in a cohort of middle-aged/late middle-aged individuals (mean 58 (interquartile range 51-64) years old).
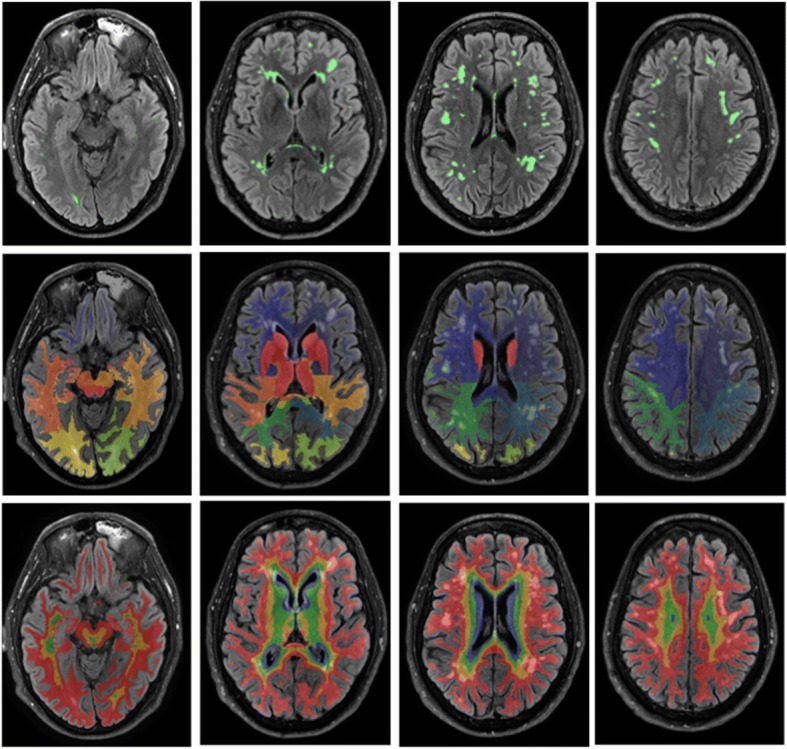
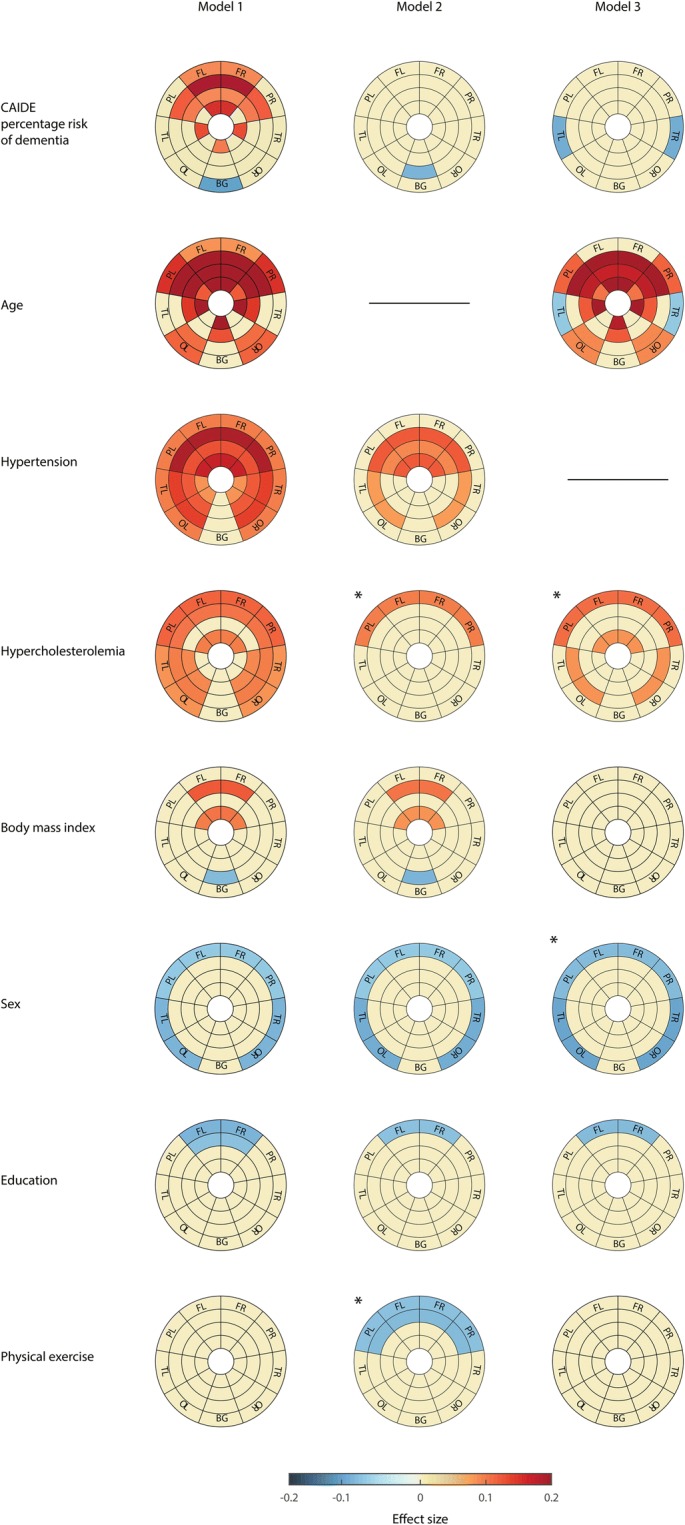
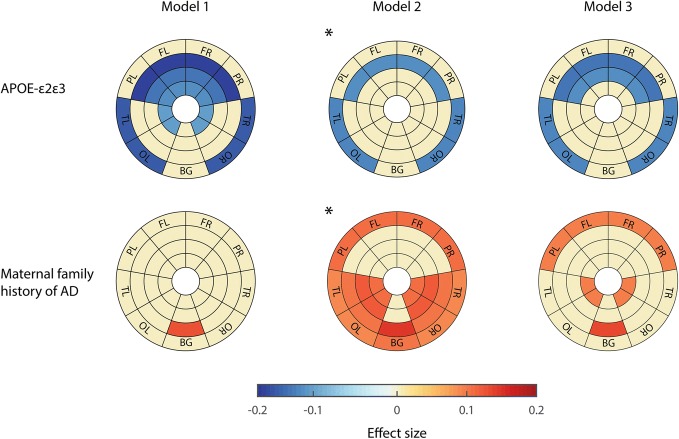
Methods: Magnetic resonance imaging and AD risk factors were collected from 575 cognitively unimpaired participants. WMH load was automatically calculated in each brain lobe and in four equidistant layers from the ventricular surface to the cortical interface. Global volumes and regional patterns of WMH load were analyzed as a function of the Cardiovascular Risk Factors, Aging and Incidence of Dementia (CAIDE) dementia risk score, as well as family history of AD and Apolipoprotein E (APOE) genotype. Additional analyses were performed after correcting for the effect of age and hypertension.
Results: The studied cohort showed very low WMH burden (median 1.94 cm3) and 20-year dementia risk estimates (median 1.47 %). Even so, higher CAIDE scores were significantly associated with increased global WMH load. The main drivers of this association were age and hypertension, with hypercholesterolemia and body mass index also displaying a minor, albeit significant, influence. Regionally, CAIDE scores were positively associated with WMH in anterior areas, mostly in the frontal lobe. Age and hypertension showed significant association with WMH in almost all regions analyzed. The APOE-ε2 allele showed a protective effect over global WMH with a pattern that comprised juxtacortical temporo-occipital and fronto-parietal deep white matter regions. Participants with maternal family history of AD had higher WMH load than those without, especially in temporal and occipital lobes.
Conclusions: WMH load is associated with AD risk factors even in cognitively unimpaired subjects with very low WMH burden and dementia risk estimates. Our results suggest that tight control of modifiable risk factors in middle-age/late middle-age could have a significant impact on late-life dementia.
Keywords: Aging; Brain; Lesions; Prevention; Vascular.
Conflict of interest statement
Ethics approval and consent to participate
The ALFA study and the MRI substudy protocols have been approved by an independent Ethics Committee Parc de Salut Mar Barcelona and registered at Clinicaltrials.gov (ALFA Identifier: NCT01835717; MRI substudy Identifier: NCT02198586). Both studies have been conducted in accordance with the directives of the Spanish Law 14/2007, of 3 July, on Biomedical Research (Ley 14/2007 de Investigación Biomédica).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- De Leeuw F-E, de Groot JC, Achten E, Oudkerk M, Ramos L, Heijboer R, et al. Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study. J Neurol Neurosurg Psychiatry. 2001;70:9–14. doi: 10.1136/jnnp.70.1.9. - DOI - PMC - PubMed
-
- Brugulat-Serrat A, Rojas S, Bargalló N, Conesa G, Minguillón C, Fauria K, et al. Incidental findings on brain MRI of cognitively normal first-degree descendants of patients with Alzheimer’s disease: a cross-sectional analysis from the ALFA (Alzheimer and Families) project. BMJ Open. 2017;7:e013215. doi: 10.1136/bmjopen-2016-013215. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
