

Remaining Hurdles for Tissue-Engineering the Temporomandibular Joint Disc
- PMID: 30678888
- PMCID: PMC6436948
- DOI: 10.1016/j.molmed.2018.12.007
Remaining Hurdles for Tissue-Engineering the Temporomandibular Joint Disc
Abstract
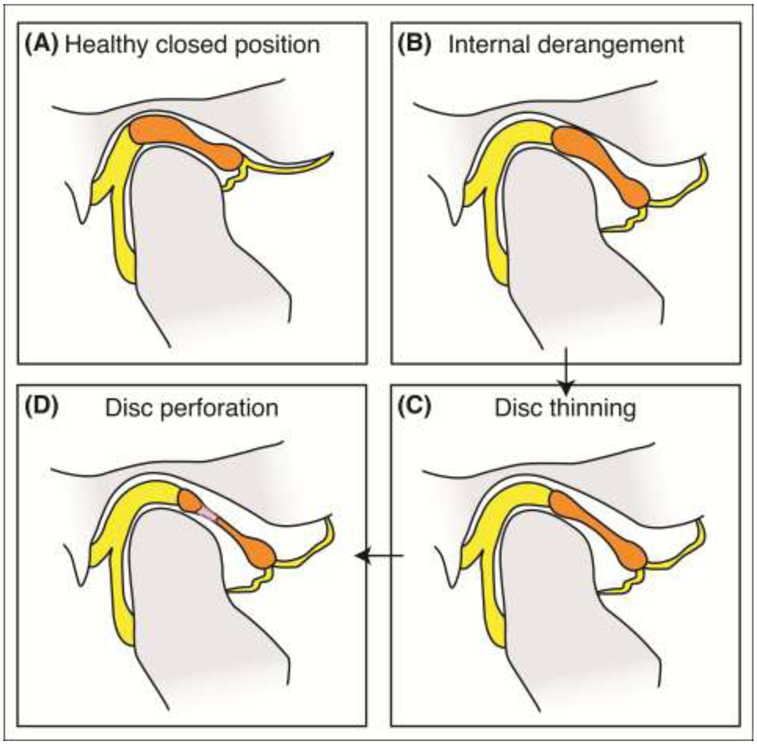
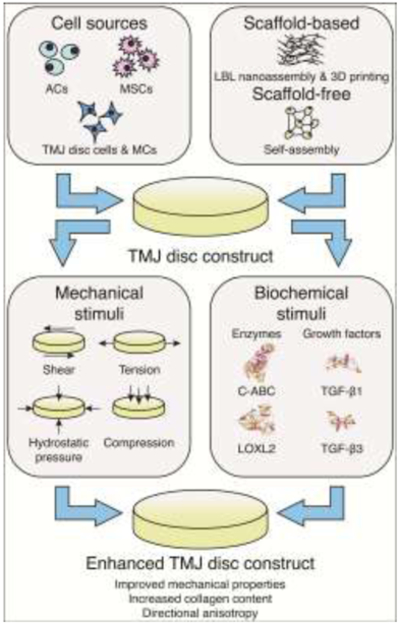
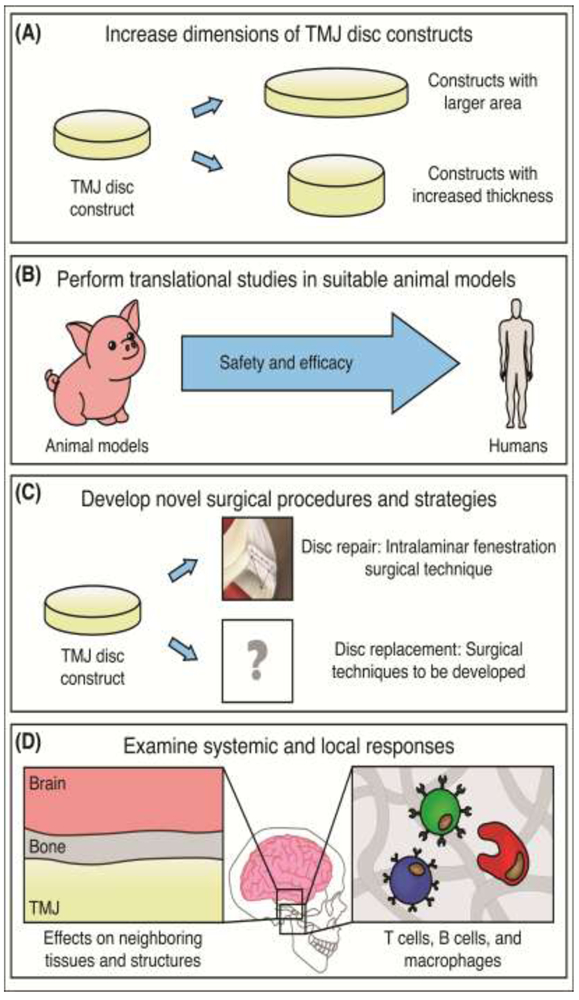
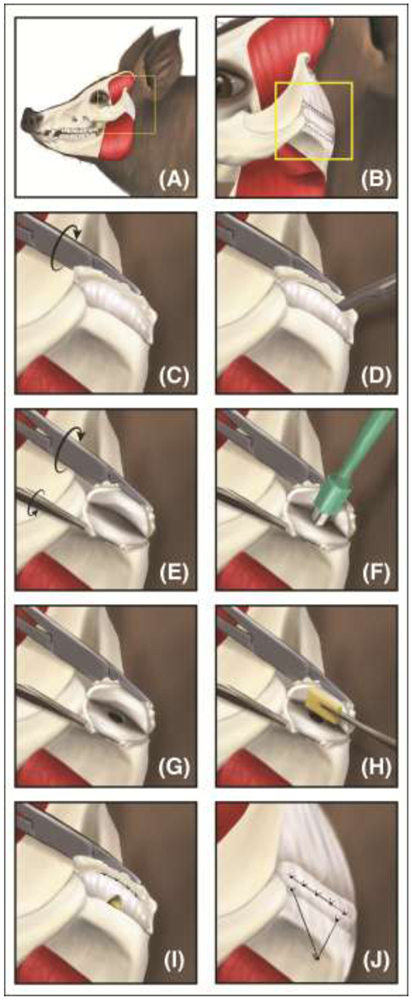
The temporomandibular joint (TMJ) disc, a fibrocartilaginous structure between the mandible and temporal bone, is implicated in temporomandibular disorders (TMDs). TMDs symptomatically affect approximately 25% of the population, of which 70% have internal derangement of the disc. Treatments lack efficiency, motivating novel therapies, including tissue-engineering toward TMJ disc regeneration. Recent developments in scaffold-based or scaffold-free approaches, cell sources, and biochemical and mechanical stimulation have resulted in constructs exhibiting native tissue mechanics. Safety and efficacy of tissue-engineered implants have shown promising results in orthotopic animal studies. However, many hurdles need to be overcome in tissue-engineering approaches, and clinical and regulatory pathways. Future studies present an opportunity for clinicians and researchers to work together toward safe and effective clinical trials.
Keywords: temporomandibular joint disc.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures

Similar articles
-
Biological Treatments for Temporomandibular Joint Disc Disorders: Strategies in Tissue Engineering.Biomolecules. 2021 Jun 23;11(7):933. doi: 10.3390/biom11070933. Biomolecules. 2021. PMID: 34201698 Free PMC article. Review.
-
Recent Tissue Engineering Advances for the Treatment of Temporomandibular Joint Disorders.Curr Osteoporos Rep. 2016 Dec;14(6):269-279. doi: 10.1007/s11914-016-0327-y. Curr Osteoporos Rep. 2016. PMID: 27704395 Free PMC article. Review.
-
[Cell sources for engineered temporomandibular joint disc tissue: present and future].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2010 Apr;27(2):463-6. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2010. PMID: 20481340 Review. Chinese.
-
A review of in-vitro fibrocartilage tissue engineered therapies with a focus on the temporomandibular joint.Arch Oral Biol. 2017 Nov;83:193-201. doi: 10.1016/j.archoralbio.2017.07.013. Epub 2017 Jul 23. Arch Oral Biol. 2017. PMID: 28787640 Free PMC article. Review.
-
The mechanics of tissue-engineered temporomandibular joint discs: Current status and prospects for enhancement.J Biomater Appl. 2024 Oct;39(4):269-287. doi: 10.1177/08853282241265059. Epub 2024 Jul 18. J Biomater Appl. 2024. PMID: 39023922 Review.
Cited by
-
Biological Treatments for Temporomandibular Joint Disc Disorders: Strategies in Tissue Engineering.Biomolecules. 2021 Jun 23;11(7):933. doi: 10.3390/biom11070933. Biomolecules. 2021. PMID: 34201698 Free PMC article. Review.
-
Therapeutic Agents for the Treatment of Temporomandibular Joint Disorders: Progress and Perspective.Front Pharmacol. 2021 Jan 29;11:596099. doi: 10.3389/fphar.2020.596099. eCollection 2020. Front Pharmacol. 2021. PMID: 33584275 Free PMC article. Review.
-
Advances in 3D printing techniques for cartilage regeneration of temporomandibular joint disc and mandibular condyle.Int J Bioprint. 2023 May 25;9(5):761. doi: 10.18063/ijb.761. eCollection 2023. Int J Bioprint. 2023. PMID: 37457936 Free PMC article. Review.
-
Bibliometric and visualization analysis of temporomandibular joint osteoarthritis from 2004 to 2024.Front Oral Health. 2025 May 30;6:1596551. doi: 10.3389/froh.2025.1596551. eCollection 2025. Front Oral Health. 2025. PMID: 40519811 Free PMC article.
-
Characterization of the Temporomandibular Joint Disc Complex in the Yucatan Minipig.Tissue Eng Part A. 2023 Aug;29(15-16):439-448. doi: 10.1089/ten.TEA.2023.0011. Epub 2023 May 29. Tissue Eng Part A. 2023. PMID: 37073459 Free PMC article.
References
-
- Alomar X et al. (2007) Anatomy of the Temporomandibular Joint. Semin. Ultrasound, CT, MRI 28, 170–183 - PubMed
-
- Sindelar BJ and Herring SW (2005) Soft tissue mechanics of the temporomandibular joint. Cells, Tissues, Organs 180, 36–43 - PubMed
-
- Arnett GW et al. (1996) Progressive mandibular retrusion-idiopathic condylar resorption. Part II. Am. J. Orthod. Dentofac. Orthopeics 110, 117–127 - PubMed
-
- Katzberg RW and Westesson P-L (1993) Diagnosis of the temporomandibular joint, (1st edn) W.B. Saunders.
