

Insights into Molecular Classifications of Triple-Negative Breast Cancer: Improving Patient Selection for Treatment
- PMID: 30679171
- PMCID: PMC6387871
- DOI: 10.1158/2159-8290.CD-18-1177
Insights into Molecular Classifications of Triple-Negative Breast Cancer: Improving Patient Selection for Treatment
Abstract
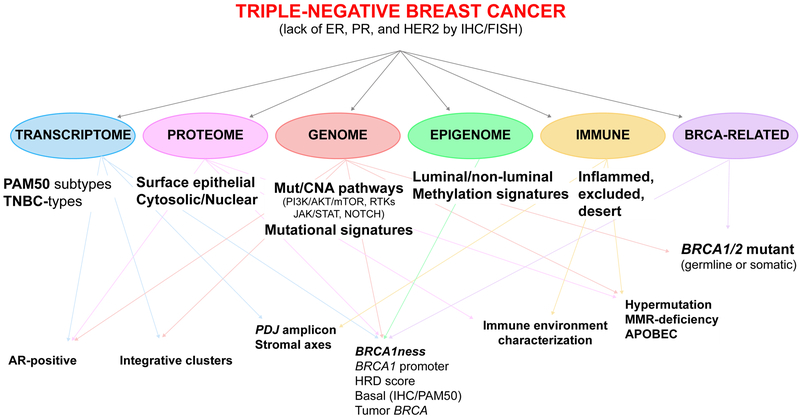
Triple-negative breast cancer (TNBC) remains the most challenging breast cancer subtype to treat. To date, therapies directed to specific molecular targets have rarely achieved clinically meaningful improvements in outcomes of patients with TNBC, and chemotherapy remains the standard of care. Here, we seek to review the most recent efforts to classify TNBC based on the comprehensive profiling of tumors for cellular composition and molecular features. Technologic advances allow for tumor characterization at ever-increasing depth, generating data that, if integrated with clinical-pathologic features, may help improve risk stratification of patients, guide treatment decisions and surveillance, and help identify new targets for drug development. SIGNIFICANCE: TNBC is characterized by higher rates of relapse, greater metastatic potential, and shorter overall survival compared with other major breast cancer subtypes. The identification of biomarkers that can help guide treatment decisions in TNBC remains a clinically unmet need. Understanding the mechanisms that drive resistance is key to the design of novel therapeutic strategies to help prevent the development of metastatic disease and, ultimately, to improve survival in this patient population.
©2019 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Bertucci F, Houlgatte R, Benziane A, Granjeaud S, Adelaide J, Tagett R, et al. Gene expression profiling of primary breast carcinomas using arrays of candidate genes. Hum Mol Genet 2000;9:2981–91. - PubMed
-
- Brown M, Tsodikov A, Bauer KR, Parise CA, Caggiano V. The role of human epidermal growth factor receptor 2 in the survival of women with estrogen and progesterone receptor-negative, invasive breast cancer: the California Cancer Registry, 1999–2004. Cancer 2008;112:737–47. - PubMed
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007;13:4429–34. - PubMed
-
- Andre F, Zielinski CC. Optimal strategies for the treatment of metastatic triple-negative breast cancer with currently approved agents. Ann Oncol 2012;23 Suppl 6:vi46–51. - PubMed
-
- Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature 2000;406:747–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
