

Trends in end digit preference for blood pressure and associations with cardiovascular outcomes in Canadian and UK primary care: a retrospective observational study
- PMID: 30679298
- PMCID: PMC6347875
- DOI: 10.1136/bmjopen-2018-024970
Trends in end digit preference for blood pressure and associations with cardiovascular outcomes in Canadian and UK primary care: a retrospective observational study
Abstract
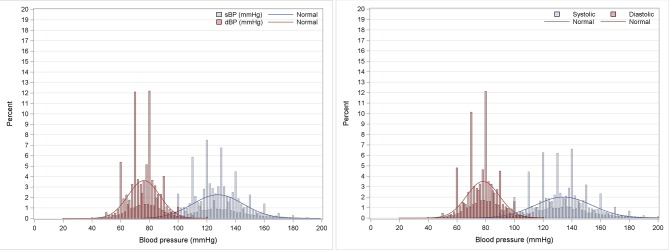
Objectives: To study systematic errors in recording blood pressure (BP) as measured by end digit preference (EDP); to determine associations between EDP, uptake of Automated Office BP (AOBP) machines and cardiovascular outcomes.
Design: Retrospective observational study using routinely collected electronic medical record data from 2006 to 2015 and a survey on year of AOBP acquisition in Toronto, Canada in 2017.
Setting: Primary care practices in Canada and the UK.
Participants: Adults aged 18 years or more.
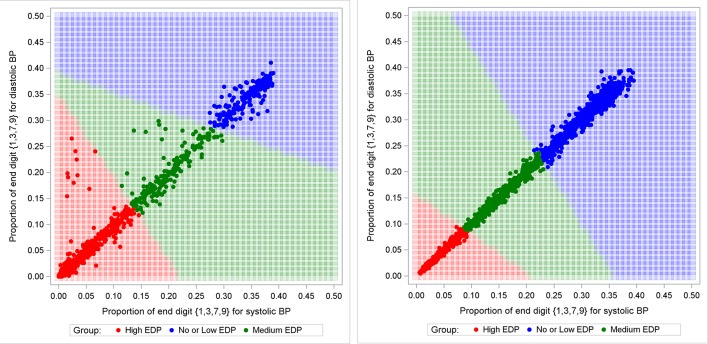
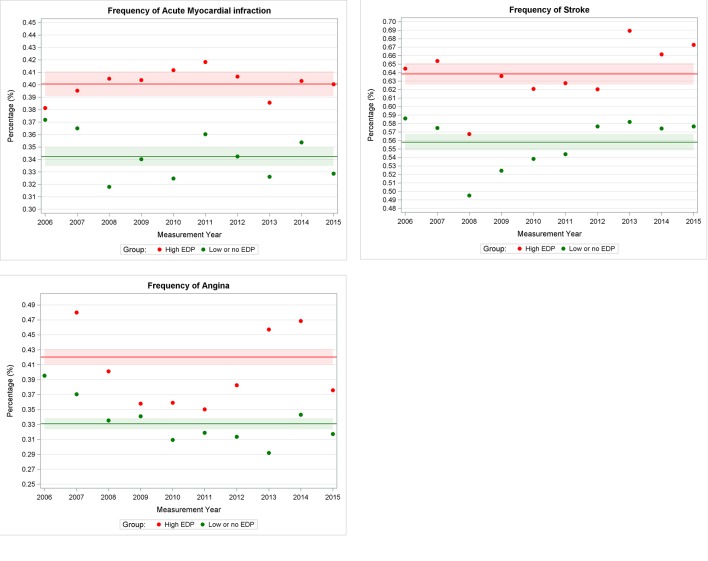
Main outcome measures: Mean rates of EDP and change in rates. Rates of EDP following acquisition of an AOBP machine. Associations between site EDP levels and mean BP. Associations between site EDP levels and frequency of cardiovascular outcomes.
Results: 707 227 patients in Canada and 1 558 471 patients in the UK were included. From 2006 to 2015, the mean rate of BP readings with both systolic and diastolic pressure ending in zero decreased from 26.6% to 15.4% in Canada and from 24.2% to 17.3% in the UK. Systolic BP readings ending in zero decreased from 41.8% to 32.5% in the 3 years following the purchase of an AOBP machine. Sites with high EDP had a mean systolic BP of 2.0 mm Hg in Canada, and 1.7 mm Hg in the UK, lower than sites with no or low EDP. Patients in sites with high levels of EDP had a higher frequency of stroke (standardised morbidity ratio (SMR) 1.15, 95% CI 1.12 to 1.17), myocardial infarction (SMR 1.16, 95% CI 1.14 to 1.19) and angina (SMR 1.25, 95% CI 1.22 to 1.28) than patients in sites with no or low EDP.
Conclusions: Acquisition of an AOBP machine was associated with a decrease in EDP levels. Sites with higher rates of EDP had lower mean BPs and a higher frequency of adverse cardiovascular outcomes. The routine use of manual office-based BP measurement should be reconsidered.
Keywords: hypertension; information technology; ischaemic heart disease; quality in health care.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- World Health Organization, global health estimates. World Health Organization. Health statistics and information systems Web site. http://www.who.int/healthinfo/global_burden_disease/en/ (Accessed 29 May 2016).
-
- Leung AA, Nerenberg K, Daskalopoulou SS, et al. . Hypertension Canada’s 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol 2016;32:569–88. 10.1016/j.cjca.2016.02.066 - DOI - PubMed
-
- Pickering TG, Hall JE, Appel LJ, et al. . Recommendations for blood pressure measurement in humans and experimental animals: Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005;45:142–61. 10.1161/01.HYP.0000150859.47929.8e - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical