

Robot-assisted Tongue Base Resection ensures favorable therapeutic outcome to Obstructive Sleep Apnea patients with Lingual tonsil hypertrophy
- PMID: 30679511
- PMCID: PMC6346104
- DOI: 10.1038/s41598-018-36800-7
Robot-assisted Tongue Base Resection ensures favorable therapeutic outcome to Obstructive Sleep Apnea patients with Lingual tonsil hypertrophy
Abstract
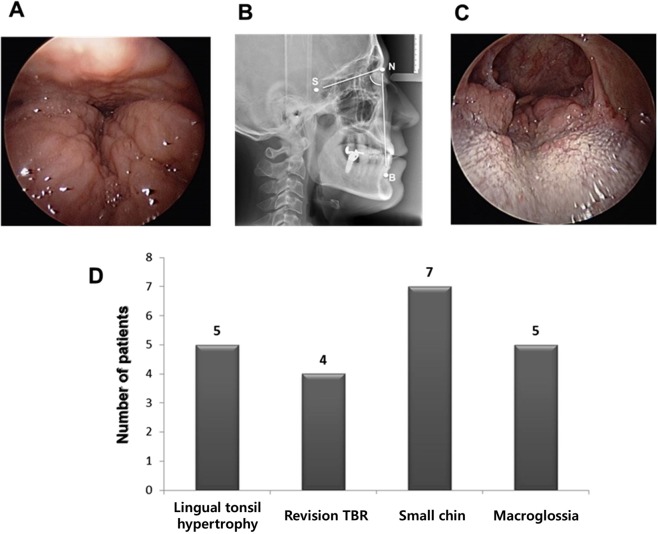
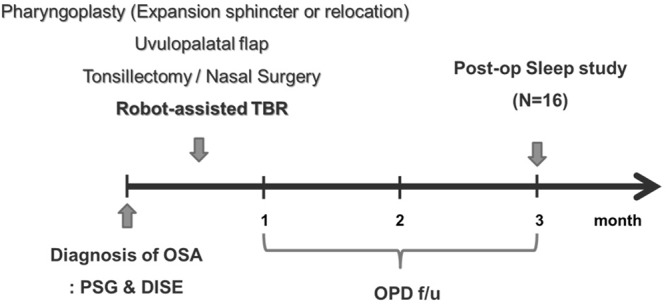
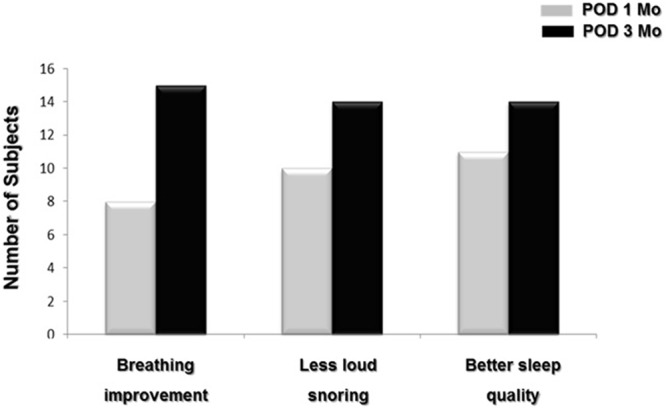
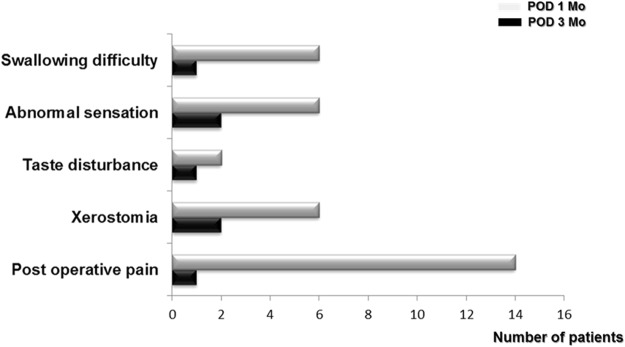
Tongue base (TB) narrowing is recognized as a significant site of upper airway collapse during sleep in obstructive sleep apnea (OSA) patients and robot technology is expected to have promising clinical utility in OSA patients with TB narrowing. The purpose of our study is to demonstrate the better therapeutic conditions and favorable indications of robot-assisted TB resection (TBR) in OSA. We performed robot-assisted TBR combined with nasal and palatal surgery in 16 OSA patients with any of the following characteristics: severe TB narrowing (over grade II) and moderate or severe OSA. The preoperative median AHI was 48.8/hr and the median lowest SaO2 was 82.0%. The median AHI decreased to 18.7/hr and ten patients (62.5%) were included in the responder group following robot-assisted TBR combined with nasal and palatal surgery. The lowest SaO2 improved to 90.5% and the posterior airway space (PAS) was significantly increased following robot-assisted TBR. Cephalometric results showed that wider PAS were observed in responders compared to non-responders prior to robot-assisted TBR. Interestingly, there was greater improvement in the objective parameters including PAS in the OSA patients with lingual tonsilar hypertrophy than they were in those without and all patients with lingual tonsillar hypertrophy (n = 6) responded to robot-assisted TBR. Robot-assisted TBR exhibited minimal morbidity and postoperative complications in OSA patients. Robot-assisted TBR can be considered a promising and innovative surgical option to reduce TB volume and improve sleep parameters in OSA patients with TB narrowing. OSA patient with TB narrowing due to lingual tonsil hypertrophy shows greater therapeutic outcome and lingual tonsil hypertrophy appears to be most favorable surgical indications of robot-assisted TBR.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Polysomnographic outcomes following lingual tonsillectomy for persistent obstructive sleep apnea in down syndrome.Laryngoscope. 2017 Feb;127(2):520-524. doi: 10.1002/lary.26202. Epub 2016 Aug 12. Laryngoscope. 2017. PMID: 27515709
-
Multi-level surgery for obstructive sleep apnea. Lingual tonsillectomy vs. hyoid suspension in combination with radiofrequency of the tongue base.Sleep Breath. 2015 Dec;19(4):1361-6. doi: 10.1007/s11325-015-1241-8. Epub 2015 Sep 9. Sleep Breath. 2015. PMID: 26354104 Clinical Trial.
-
Robotic Tongue-Base Resection Combined With Tongue-Base Suspension for Obstructive Sleep Apnea.Laryngoscope. 2020 Sep;130(9):2285-2291. doi: 10.1002/lary.28443. Epub 2019 Nov 29. Laryngoscope. 2020. PMID: 31782809
-
Surgical Management of Pediatric Obstructive Sleep Apnea Beyond Tonsillectomy & Adenoidectomy: Tongue Base and Larynx.Otolaryngol Clin North Am. 2024 Jun;57(3):431-445. doi: 10.1016/j.otc.2024.02.005. Epub 2024 Mar 23. Otolaryngol Clin North Am. 2024. PMID: 38523050 Review.
-
Pediatric lingual tonsillectomy.Adv Otorhinolaryngol. 2012;73:109-11. doi: 10.1159/000334459. Epub 2012 Mar 29. Adv Otorhinolaryngol. 2012. PMID: 22472240 Review.
Cited by
-
Transoral Robotic Surgery for Patients with Obstructive Sleep Apnoea: A Systematic Literature Review of Current Practices.Life (Basel). 2024 Dec 22;14(12):1700. doi: 10.3390/life14121700. Life (Basel). 2024. PMID: 39768406 Free PMC article. Review.
-
Feasibility of transoral robotic surgery using the da Vinci Xi system for oropharyngeal cancer and obstructive sleep apnea in low-volume center.J Robot Surg. 2024 Nov 7;18(1):398. doi: 10.1007/s11701-024-02155-7. J Robot Surg. 2024. PMID: 39508908 Review.
-
Sleep parameter characteristics of patients with OSA who have retropalatal circumferential narrowing and the clinical significance of lateral pharyngeal wall collapse during sleep.Sleep Breath. 2023 Dec;27(6):2165-2173. doi: 10.1007/s11325-023-02808-1. Epub 2023 Mar 24. Sleep Breath. 2023. PMID: 36959432 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
