

Association between preterm delivery and bacterial vaginosis with or without treatment
- PMID: 30679584
- PMCID: PMC6345902
- DOI: 10.1038/s41598-018-36964-2
Association between preterm delivery and bacterial vaginosis with or without treatment
Abstract
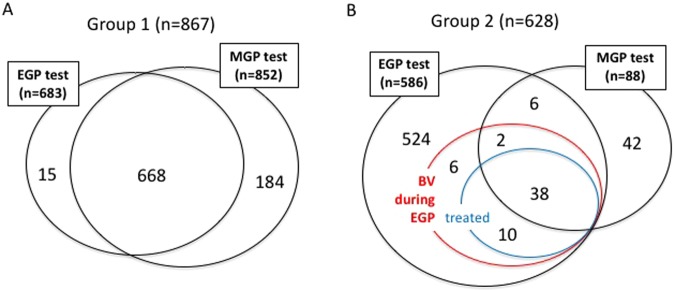
The relationship between bacterial vaginosis (BV) and preterm delivery has become well known in recent years, although there are few studies on: (i) the differences in test results during the early gestational (EGP) and middle gestational (MGP) periods; (ii) the significance of the intermediate (I) group that does not develop overt BV; or (iii) the therapeutic effects of metronidazole. We performed a retrospective study to analyze the relationship between the vaginal bacterial status and the preterm delivery rate. Without treatment, the preterm delivery rate was higher in the BV subgroup than in the I and normal (N) subgroups (p = 0.021) in the EGP, whereas the rates in the BV and I subgroups were higher than in the N subgroup in the MGP (p = 0.0003). Although treatment of BV by metronidazole vaginal tablets significantly increased the N subgroup in the MGP (p = 0.020), there was no significant improvement in the preterm delivery rate. Decreasing the rate of preterm delivery requires development of treatment methods that will further increase the percentage of patients who test N during the MGP after BV during the EGP.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Hibbard JU, Hibbard MC, Ismail M, Arendt E. Pregnancy outcome after expectant management of premature rupture of the membranes in the second trimester. J. Reprod. Med. 1993;38:945–951. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
