

Comparative study in leg telangiectasias treatment with Nd:YAG laser and sclerotherapy
- PMID: 30679981
- PMCID: PMC6327418
- DOI: 10.3892/etm.2018.6985
Comparative study in leg telangiectasias treatment with Nd:YAG laser and sclerotherapy
Abstract
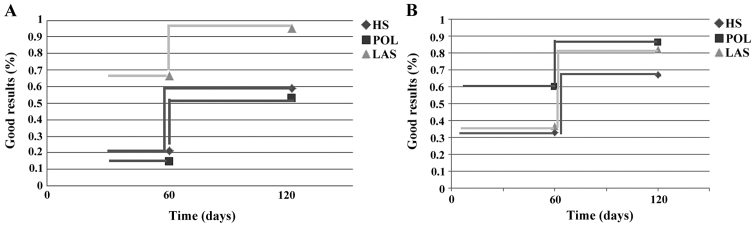
Telangiectasias and reticular veins of the lower extremities are common lesions. Sclerotherapy is considered the gold standard for treatment. The aim of our prospective randomized study was to compare the efficacy and safety of hypertonic 20% saline/2% lignocaine (HS) versus polidocanol 0.5% (POL) versus long-pulsed neodymium:ytrium aluminium garnet (Nd:YAG) laser (LAS) treatments of leg telangiectasias in women, using each patient as her own control. We included in this study 285 women with primary leg telangiectasias and reticular veins (C1AEpAS1PN) in order to be treated with sclerotherapy or laser. One leg was treated with either LAS, POL or HS. The other leg received, randomly, one other of these treatments. At the end there were 190 legs treated with each method. There were two sessions at 8-week interval. Assessment of vessel clearing and complications was conducted 2 months after each session using before and after photographs of the leg vessels using a six-point scale from 0 (no change) to 5 (100% cleared). For telangiectasias under 1 mm diameter LAS was better (RR=9.72, P<0.0001) than HS and also POL was better (RR=2.70, P=0.003); for telangiectasias over 1 mm diameter LAS and POL were better too (RR=2.70, P=0.003) respectively (RR=1.44, P=0.00756). For telangiectasias under 1 mm LAS treatment is clearly superior to POL treatment. For telangiectasias over 1 mm the hazard regression model showed a hazard ratio of 3.97 (P=0.047) for LAS and 4.96 (P=0.486) for POL vs. HS treatment. In conclusion, telangiectasias and reticular veins of the lower extremities can be successfully treated with Nd:YAG laser or sclerotherapy. Nd:YAG laser is recommended in treating small telangiectasias (under 1 mm diameter) while sclerotherapy with polidocanol is more efficient as long as telangiectasias diameter is growing.
Keywords: laser; sclerotherapy; telangiectasias treatment.
Figures
Similar articles
-
Single Blind, Randomised Study Regarding the Treatment of the Telangiectasia of the Lower Limbs (C1EAP) Using Polidocanol 0,5%, 1%, and Nd:YAG Laser.Curr Health Sci J. 2020 Apr-Jun;46(2):141-149. doi: 10.12865/CHSJ.46.02.07. Epub 2020 Jun 30. Curr Health Sci J. 2020. PMID: 32874686 Free PMC article.
-
Treatment of lower extremity telangiectasias in women by foam sclerotherapy vs. Nd:YAG laser: a prospective, comparative, randomized, open-label trial.J Eur Acad Dermatol Venereol. 2015 Mar;29(3):549-54. doi: 10.1111/jdv.12627. Epub 2014 Jul 28. J Eur Acad Dermatol Venereol. 2015. PMID: 25069999 Clinical Trial.
-
Comparison and sequential study of long pulsed Nd:YAG 1,064 nm laser and sclerotherapy in leg telangiectasias treatment.Lasers Surg Med. 2004;34(3):273-6. doi: 10.1002/lsm.20010. Lasers Surg Med. 2004. PMID: 15022257
-
Transcutaneous laser treatment of leg veins.Lasers Med Sci. 2014 Mar;29(2):481-92. doi: 10.1007/s10103-013-1483-2. Epub 2013 Nov 13. Lasers Med Sci. 2014. PMID: 24220848 Review.
-
Optimal parameters for the treatment of leg veins using Nd:YAG lasers at 1064 nm.Br J Dermatol. 2006 Aug;155(2):364-71. doi: 10.1111/j.1365-2133.2006.07314.x. Br J Dermatol. 2006. PMID: 16882176 Review.
Cited by
-
The Second Conference of the Romanian Society of Immuno-Dermatology, Bucharest, September 27-29, 2018.Exp Ther Med. 2019 Feb;17(2):979-981. doi: 10.3892/etm.2018.7067. Epub 2018 Dec 6. Exp Ther Med. 2019. PMID: 30679962 Free PMC article. No abstract available.
-
Pharmacological Properties of Chalcones: A Review of Preclinical Including Molecular Mechanisms and Clinical Evidence.Front Pharmacol. 2021 Jan 18;11:592654. doi: 10.3389/fphar.2020.592654. eCollection 2020. Front Pharmacol. 2021. PMID: 33536909 Free PMC article. Review.
-
Treatment for telangiectasias and reticular veins.Cochrane Database Syst Rev. 2021 Oct 12;10(10):CD012723. doi: 10.1002/14651858.CD012723.pub2. Cochrane Database Syst Rev. 2021. PMID: 34637138 Free PMC article.
-
Single Blind, Randomised Study Regarding the Treatment of the Telangiectasia of the Lower Limbs (C1EAP) Using Polidocanol 0,5%, 1%, and Nd:YAG Laser.Curr Health Sci J. 2020 Apr-Jun;46(2):141-149. doi: 10.12865/CHSJ.46.02.07. Epub 2020 Jun 30. Curr Health Sci J. 2020. PMID: 32874686 Free PMC article.
-
Brazilian guidelines on chronic venous disease of the Brazilian Society of Angiology and Vascular Surgery.J Vasc Bras. 2023 Nov 6;22:e20230064. doi: 10.1590/1677-5449.202300642. eCollection 2023. J Vasc Bras. 2023. PMID: 38021274 Free PMC article.
References
-
- Tudoraşcu I, Sfredel V, Riza AL, Miulescu Dănciulescu R, Ianoşi SL, Dănoiu S. Motor unit changes in normal aging: A brief review. Rom J Morphol Embryol. 2014;55:1295–1301. - PubMed
-
- Heck M, Faulhaber J, Breu FX, Schneider SW. Foam sclerotherapy. Uses and indications in dermatology and phlebology. Hautarzt. 2012;63:493–505. (In German) - PubMed
-
- Perrin M, Eklof B, VAN Rij A, Labropoulos N, Vasquez M, Nicolaides A, Blattler W, Bouhassira D, Bouskela E, Carpentier P, et al. Venous symptoms: The SYM Vein Consensus statement developed under the auspices of the European Venous Forum. Int Angiol. 2016;35:374–398. - PubMed
LinkOut - more resources
Full Text Sources
Medical