

Neurologic Outcomes in a Two-Center Cohort of Neonatal and Pediatric Patients Supported on Extracorporeal Membrane Oxygenation
- PMID: 30681441
- PMCID: PMC7765760
- DOI: 10.1097/MAT.0000000000000933
Neurologic Outcomes in a Two-Center Cohort of Neonatal and Pediatric Patients Supported on Extracorporeal Membrane Oxygenation
Abstract
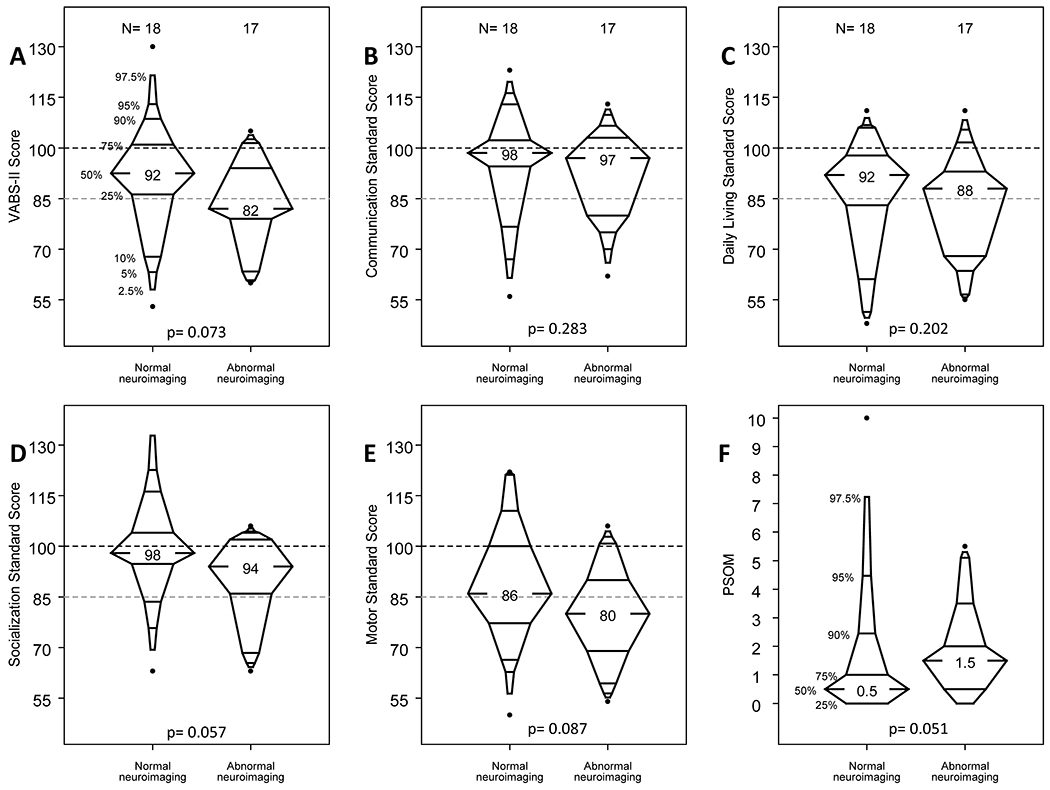
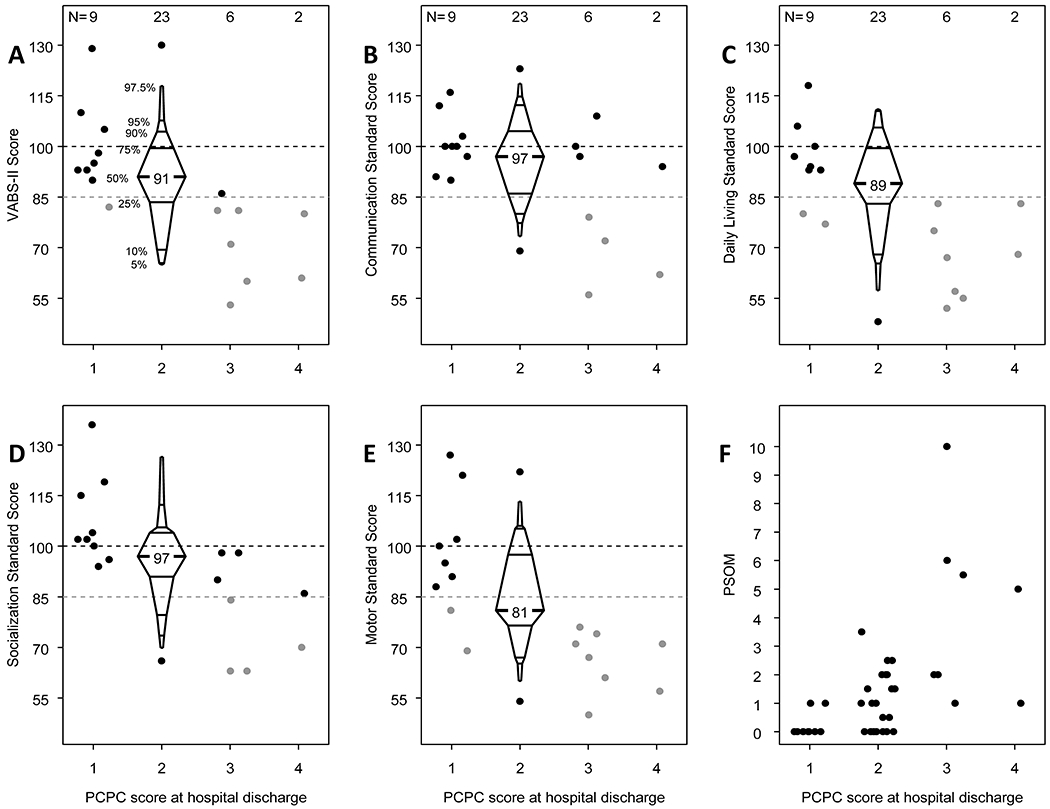
Contemporary studies of long-term outcomes in children supported on extracorporeal membrane oxygenation (ECMO) in the United States are limited. We enrolled 99 ECMO patients between July 2010 and June 2015 in a two-center prospective observational study that included neurologic and neuropsychologic evaluation at 6 and 12 months, using standardized outcome measures. Pre-ECMO, 20 (20%) had a pre-existing neurologic diagnosis, 40 (40%) had cardiac arrest, and 10 of 47 (21%) children with neuroimaging had acute abnormal findings. Of 50 children eligible for follow-up at 6 or 12 months, 40 (80%) returned for at least one visit. At the follow-up visit of longest interval from ECMO, the median Vineland Adaptive Behavior Scales-II (VABS-II) score was 91 (interquartile range [IQR], 81-98), the median Pediatric Stroke Outcome Measure (PSOM) score was 1 (IQR, 0-2), and the median Mullen Scales of Early Learning composite score was 85 (IQR, 72-96). Presence of new neuroimaging abnormalities during ECMO or within 6 weeks post-ECMO was associated with VABS-II score <85 or death within 12 months after ECMO. The Pediatric Cerebral Performance Category at hospital discharge showed a strong relationship with unfavorable VABS-II and PSOM scores at 6 or 12 months after ECMO. In this study, we report a higher prevalence of pre-ECMO neurologic conditions than previously described. In survivors to hospital discharge, median scores for adaptive behavior and cognitive, neurologic, and quality of life assessments were all below the general population means, but most deficits would be considered minor within each of the domains tested.
Figures

Comment in
-
Neurodevelopmental Outcomes in Pediatric Extracorporeal Membrane Oxygenation.ASAIO J. 2020 Jan;66(1):89-90. doi: 10.1097/MAT.0000000000001112. ASAIO J. 2020. PMID: 31860610 No abstract available.
References
-
- Hill JD, O’Brien TG, Murray JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). use of the bramson membrane lung. N Engl J Med. 1972;286(12):629–634. - PubMed
-
- Thiagarajan RR, Barbaro RP, Rycus PT, et al. Extracorporeal life support organization registry international report 2016. ASAIO J. 2017;63(1):60–67. - PubMed
-
- Thiagarajan RR, Laussen PC, Rycus PT, Bartlett RH, Bratton SL. Extracorporeal membrane oxygenation to aid cardiopulmonary resuscitation in infants and children. Circulation. 2007;116(15):1693–1700. - PubMed
-
- Barrett CS, Bratton SL, Salvin JW, Laussen PC, Rycus PT, Thiagarajan RR. Neurological injury after extracorporeal membrane oxygenation use to aid pediatric cardiopulmonary resuscitation. Pediatr Crit Care Med. 2009;10(4):445–451. - PubMed
-
- Weber TR, Kountzman B. Extracorporeal membrane oxygenation for nonneonatal pulmonary and multiple-organ failure. J Pediatr Surg. 1998;33(11):1605–1609. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
