

Effect of Implementing Discharge Readiness Assessment in Adult Medical-Surgical Units on 30-Day Return to Hospital: The READI Randomized Clinical Trial
- PMID: 30681712
- PMCID: PMC6484543
- DOI: 10.1001/jamanetworkopen.2018.7387
Effect of Implementing Discharge Readiness Assessment in Adult Medical-Surgical Units on 30-Day Return to Hospital: The READI Randomized Clinical Trial
Abstract
Importance: The downward trend in readmissions has recently slowed. New enhancements to hospital readmission reduction efforts are needed. Structured assessment of patient readiness for discharge has been recommended as an addition to discharge preparation standards of care to assist with tailoring of risk-mitigating actions.
Objective: To determine the effect of unit-based implementation of readiness evaluation and discharge intervention protocols on readmissions and emergency department or observation visits.
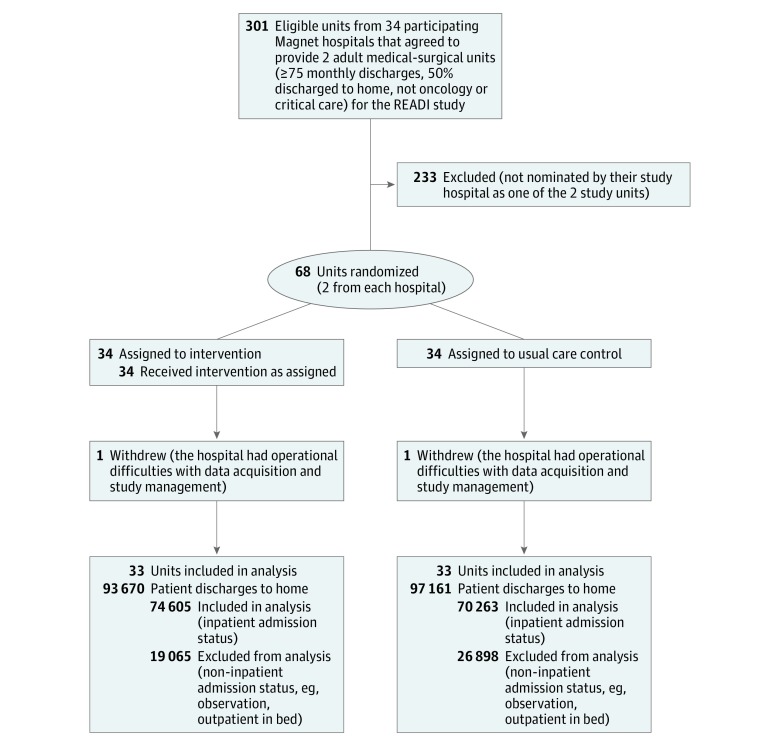
Design, setting, and participants: The Readiness Evaluation and Discharge Interventions (READI) cluster randomized clinical trial conducted in medical-surgical units of 33 Magnet hospitals between September 15, 2014, and March 31, 2017, included all adult (aged ≥18 years) patients discharged to home. Baseline and risk-adjusted intent-to-treat analyses used difference-in-differences multilevel logistic regression models with controls for patient characteristics.
Interventions: Of 2 adult medical-surgical nursing units from each hospital, 1 was randomized to the intervention and 1 to usual care conditions. Using the 8-item Readiness for Hospital Discharge Scale, the 33 intervention units implemented a sequence of protocols with increasing numbers of components: READI1, in which nurses assessed patients to inform discharge preparation; READI2, which added patient self-assessment; and READI3, which added an instruction to act on a specified Readiness for Hospital Discharge Scale cutoff score indicative of low readiness.
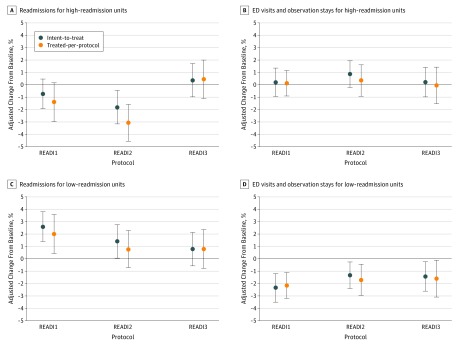
Main outcomes and measures: Thirty-day return to hospital (readmission or emergency department and observation visits). Intervention units above median baseline readmission rate (>11.3%) were categorized as high-readmission units. Among the 33 intervention units, 17 were low-readmission units and 16 were high-readmission units.
Results: The sample included 144 868 patient discharges (mean [SD] age, 59.6 [17.5] years; 51% female; 74 605 in the intervention group and 70 263 in the control group); 17 667 (12.2%) were readmitted and 12 732 (8.8%) had an emergency department visit or observation stay. None of the READI protocols reduced the primary outcome of return to hospital in intent-to-treat analysis of the full sample. In exploratory subgroup analysis, when patient self-assessments were combined with readiness assessment by nurses (READI2), readmissions were reduced by 1.79 percentage points (95% CI, -3.20 to -0.40 percentage points; P = .009) on high-readmission units. With nurse assessment alone and on low-readmission units, results were mixed.
Conclusions and relevance: Implemented in a broad range of hospitals and patients, the READI interventions were not effective in reducing return to hospital. However, adding a structured discharge readiness assessment that incorporates the patient's own perspective to usual discharge care practices holds promise for mitigating high rates of return to the hospital following discharge.
Trial registration: ClinicalTrials.gov Identifier: NCT01873118.
Conflict of interest statement
Figures
Similar articles
-
Individual Nurse Productivity in Preparing Patients for Discharge Is Associated With Patient Likelihood of 30-Day Return to Hospital.Med Care. 2019 Sep;57(9):688-694. doi: 10.1097/MLR.0000000000001170. Med Care. 2019. PMID: 31335757 Free PMC article.
-
Nurse and patient perceptions of discharge readiness in relation to postdischarge utilization.Med Care. 2010 May;48(5):482-6. doi: 10.1097/MLR.0b013e3181d5feae. Med Care. 2010. PMID: 20393364
-
Nurse Continuity at Discharge and Return to Hospital.Nurs Res. 2020 May/Jun;69(3):186-196. doi: 10.1097/NNR.0000000000000417. Nurs Res. 2020. PMID: 31934945 Clinical Trial.
-
Impact of Pharmacist-led Discharge Counseling on Hospital Readmission and Emergency Department Visits: A Systematic Review and Meta-analysis.J Hosp Med. 2020 Jan 1;15(1):52-59. doi: 10.12788/jhm.3182. Epub 2019 Mar 20. J Hosp Med. 2020. PMID: 30897055
-
Interventions to Improve Communication at Hospital Discharge and Rates of Readmission: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Aug 2;4(8):e2119346. doi: 10.1001/jamanetworkopen.2021.19346. JAMA Netw Open. 2021. PMID: 34448868 Free PMC article.
Cited by
-
Ready to Go Home? Assessment of Shared Mental Models of the Patient and Discharging Team Regarding Readiness for Hospital Discharge.J Hosp Med. 2021 Jun;16(6):326-332. doi: 10.12788/jhm.3464. J Hosp Med. 2021. PMID: 33357321 Free PMC article.
-
Theoretical concepts and instruments for measuring hospital discharge readiness: A scoping review.Heliyon. 2024 Feb 21;10(5):e26554. doi: 10.1016/j.heliyon.2024.e26554. eCollection 2024 Mar 15. Heliyon. 2024. PMID: 38439820 Free PMC article.
-
Routine provision of feedback from patient-reported outcome measurements to healthcare providers and patients in clinical practice.Cochrane Database Syst Rev. 2021 Oct 12;10(10):CD011589. doi: 10.1002/14651858.CD011589.pub2. Cochrane Database Syst Rev. 2021. PMID: 34637526 Free PMC article.
-
Impact of Social Risk Screening on Discharge Care Processes and Postdischarge Outcomes: A Pragmatic Mixed-Methods Clinical Trial During the COVID-19 Pandemic.Med Care. 2024 Oct 1;62(10):639-649. doi: 10.1097/MLR.0000000000002048. Epub 2024 Sep 6. Med Care. 2024. PMID: 39245813 Free PMC article. Clinical Trial.
-
Feasibility and Acceptability of a mHealth Self-Management Intervention for Pediatric Transplant Families.West J Nurs Res. 2022 Oct;44(10):955-965. doi: 10.1177/01939459211024656. Epub 2021 Jun 21. West J Nurs Res. 2022. PMID: 34154460 Free PMC article.
References
-
- Medicare Payment Advisory Commission Report to the Congress: Medicare and Health Care Delivery System Washington, DC: Medicare Payment Advisory Commission; 2018. http://medpac.gov/docs/default-source/reports/jun18_medpacreporttocongre.... Accessed September 20, 2018.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
