

Which osteoarthritic gait features recover following total knee replacement surgery?
- PMID: 30682010
- PMCID: PMC6347391
- DOI: 10.1371/journal.pone.0203417
Which osteoarthritic gait features recover following total knee replacement surgery?
Abstract
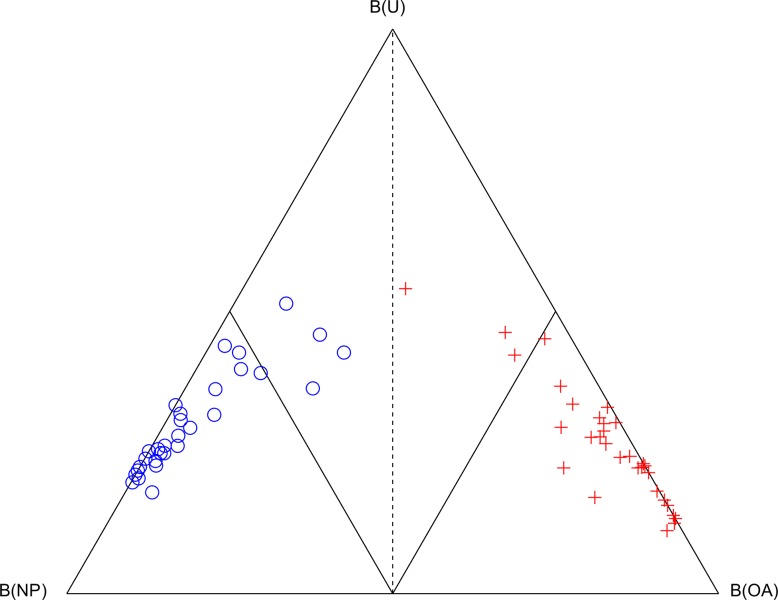
Background: Gait analysis can be used to measure variations in joint function in patients with knee osteoarthritis (OA), and is useful when observing longitudinal biomechanical changes following Total Knee Replacement (TKR) surgery. The Cardiff Classifier is an objective classification tool applied previously to examine the extent of biomechanical recovery following TKR. In this study, it is further developed to reveal the salient features that contribute to recovery towards healthy function.
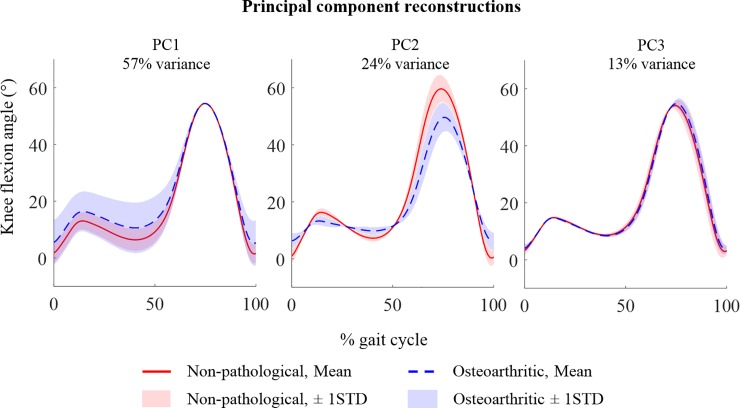
Methods: Gait analysis was performed on 30 patients before and after TKR surgery, and 30 healthy controls. Median TKR follow-up time was 13 months. The combined application of principal component analysis (PCA) and the Cardiff Classifier defined 18 biomechanical features that discriminated OA from healthy gait. Statistical analysis tested whether these features were affected by TKR surgery and, if so, whether they recovered to values found for the controls.
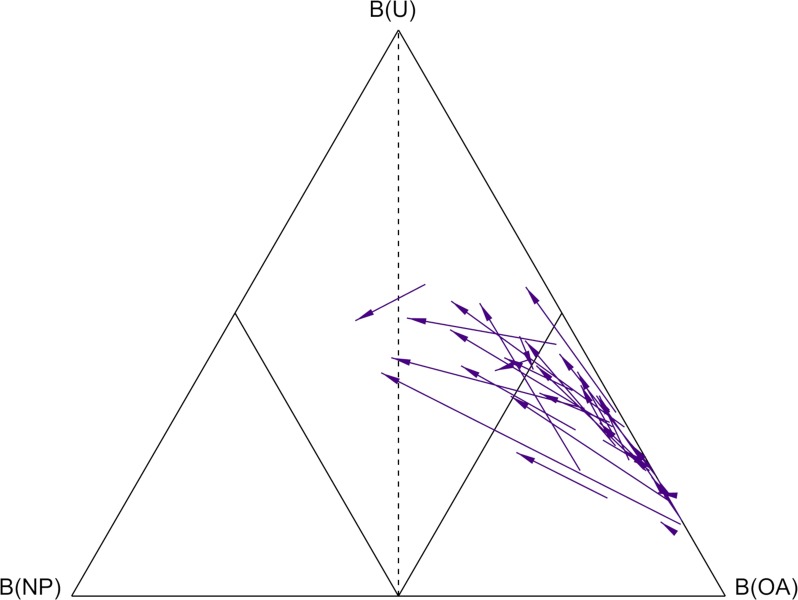
Results: The Cardiff Classifier successfully discriminated between OA and healthy gait in all 60 cases. Of the 18 discriminatory features, only six (33%) were significantly affected by surgery, including features in all three planes of the ground reaction force (p<0.001), ankle dorsiflexion moment (p<0.001), hip adduction moment (p = 0.003), and transverse hip angle (p = 0.007). All but two (89%) of these features remained significantly different to those of the control group after surgery.
Conclusions: This approach was able to discriminate gait biomechanics associated with knee OA. The ground reaction force provided the strongest discriminatory features. Despite increased gait velocity and improvements in self-reported pain and function, which would normally be clinical indicators of recovery, the majority of features were not affected by TKR surgery. This TKR cohort retained pre-operative gait patterns; reduced sagittal hip and knee moments, decreased knee flexion, increased hip flexion, and reduced hip adduction. The changes that were associated with surgery were predominantly found at the ankle and hip, rather than at the knee.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Correlations between patient-perceived outcome and objectively-measured biomechanical change following Total Knee Replacement.Gait Posture. 2019 May;70:65-70. doi: 10.1016/j.gaitpost.2019.02.028. Epub 2019 Feb 25. Gait Posture. 2019. PMID: 30826689 Free PMC article. Clinical Trial.
-
Hip, Knee, and Ankle Osteoarthritis Negatively Affects Mechanical Energy Exchange.Clin Orthop Relat Res. 2016 Sep;474(9):2055-63. doi: 10.1007/s11999-016-4921-1. Epub 2016 Jun 10. Clin Orthop Relat Res. 2016. PMID: 27287859 Free PMC article.
-
Biomechanical changes at the hip, knee, and ankle joints during gait are associated with knee osteoarthritis severity.J Orthop Res. 2008 Mar;26(3):332-41. doi: 10.1002/jor.20496. J Orthop Res. 2008. PMID: 17960658
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
Proximal gait adaptations in individuals with knee osteoarthritis: A systematic review and meta-analysis.J Biomech. 2019 Apr 18;87:127-141. doi: 10.1016/j.jbiomech.2019.02.027. Epub 2019 Mar 11. J Biomech. 2019. PMID: 30904334
Cited by
-
Effectiveness of Early Rehabilitation with Exergaming in Virtual Reality on Gait in Patients after Total Knee Replacement.J Clin Med. 2022 Aug 23;11(17):4950. doi: 10.3390/jcm11174950. J Clin Med. 2022. PMID: 36078879 Free PMC article.
-
Changes in frontal plane kinematics over 12-months in individuals with the Percutaneous Osseointegrated Prosthesis (POP).PLoS One. 2023 Feb 22;18(2):e0281339. doi: 10.1371/journal.pone.0281339. eCollection 2023. PLoS One. 2023. PMID: 36812173 Free PMC article.
-
Investigating and defining outcomes of suprapatellar versus infrapatellar intramedullary nailing of tibial shaft fractures: a protocol for a pilot randomised controlled trial.Pilot Feasibility Stud. 2022 May 26;8(1):110. doi: 10.1186/s40814-022-01057-5. Pilot Feasibility Stud. 2022. PMID: 35619162 Free PMC article.
-
Can the Output of a Learned Classification Model Monitor a Person's Functional Recovery Status Post-Total Knee Arthroplasty?Sensors (Basel). 2022 May 12;22(10):3698. doi: 10.3390/s22103698. Sensors (Basel). 2022. PMID: 35632107 Free PMC article.
-
Gait speed and kinesiophobia explain physical activity level in adults with osteoarthritis: A cross-sectional study.J Orthop Res. 2023 Dec;41(12):2629-2637. doi: 10.1002/jor.25624. Epub 2023 May 31. J Orthop Res. 2023. PMID: 37254645 Free PMC article.
References
-
- Losina E, Katz J. Total knee arthroplasty on the rise in younger patients: are we sure that past performance will guarantee future success? Arthritis Rheumatol. 2012; Available: http://onlinelibrary.wiley.com/doi/10.1002/art.33371/full - DOI - PMC - PubMed
-
- Nilsdotter AAK, Toksvig-Larsen S, Roos EEM. Knee arthroplasty: are patients’ expectations fulfilled? A prospective study of pain and function in 102 patients with 5-year follow-up. Acta Orthop. 2009;80: 55–61. Available: http://www.tandfonline.com/doi/abs/10.1080/17453670902805007 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
